THE LEUKEMIAS AND LYMPHOMAS:
The leukemias are a group of malignant neoplasms of blood and blood-forming organs, including the bone marrow, the spleen, and the lymph nodes. Abnormal numbers and uncontrolled clonal proliferation of specific types of blood cells in the myeloid or lymphoid cell lines are seen and are characteristic of the leukemias. Too many leukemic cells result in bone marrow overcrowding, reducing the normal production and function of blood cells. Because there is often a decrease of normal, functional erythrocytes, neutrophils and platelets, this leads to abnormalities in blood clotting, anemia, and frequent infections.
Leukemias are named and classified by the cell line and cell type that is affected, as well as how much the neoplastic cells have differentiated. Acute leukemias are characterized by large, immature, hematopoietic cells called blasts, and illness tends to come on suddenly and progress quickly. Chronic leukemias are characterized by more mature, somewhat functional cells and illness tends to come on or progress more slowly. Many chronic leukemias, however, can become acute and vice versa.
Leukemias are named and classified by the cell line and cell type that is affected, as well as how much the neoplastic cells have differentiated. Acute leukemias are characterized by large, immature, hematopoietic cells called blasts, and illness tends to come on suddenly and progress quickly. Chronic leukemias are characterized by more mature, somewhat functional cells and illness tends to come on or progress more slowly. Many chronic leukemias, however, can become acute and vice versa.
Types of Leukemias and Lymphomas:
- Acute Lymphocytic Leukemia (ALL)
- Acute Myeloid Leukemia (AML)
- Chronic Lymphocytic Leukemia (CLL)
- Chronic Myeloid Leukemia (CML)
- Hairy Cell Leukemia
- B-Cell Leukemia (B-CLL)
- Multiple Myeloma
- Myelodysplastic Syndrome
- Hodgkin' Lymphoma
- Non-Hodgkin's Lymphoma
- Burkitt's Lymphoma
When it comes to mature lymphoproliferative disorders, treatment is typically for the complications of the disease, and almost all blasts are in the bone marrow. Damaged cells, smudge cells, or basket cells may be seen. The survival rate is about 10 years on average, and the age group is generally older (>50 years of age). Frequent infections are common.
The Bone Marrow:
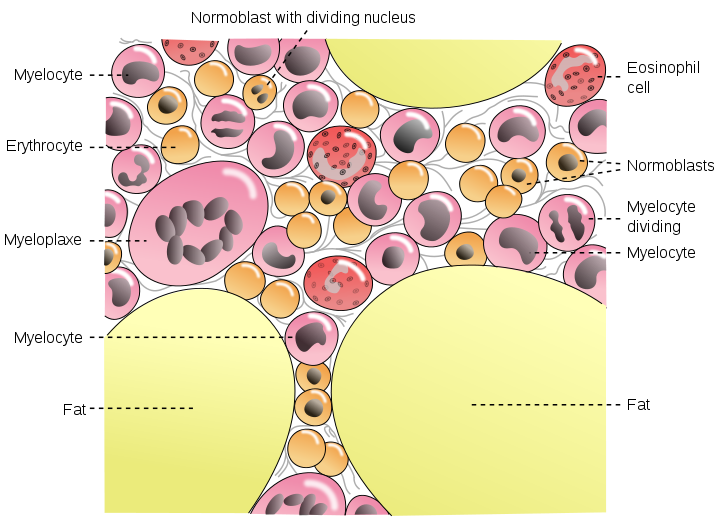
By Mysid - Vectorized by Mysid Inkscape, based on plate 72 from Gray's Anatomy (1918, public domain)., Public Domain, https://commons.wikimedia.org/w/index.php?curid=10486637
The Spleen:
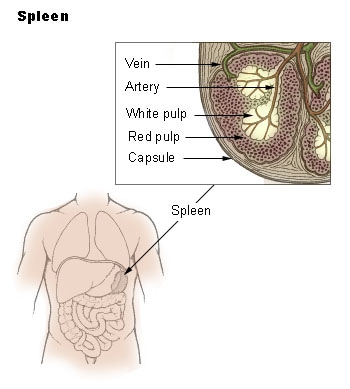
Public Domain, https://commons.wikimedia.org/w/index.php?curid=1394146
The Lymph Nodes:
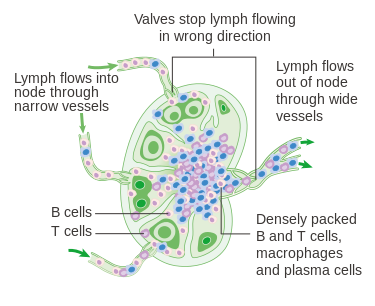
By Cancer Research UK - Original email from CRUK, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=34332684
|
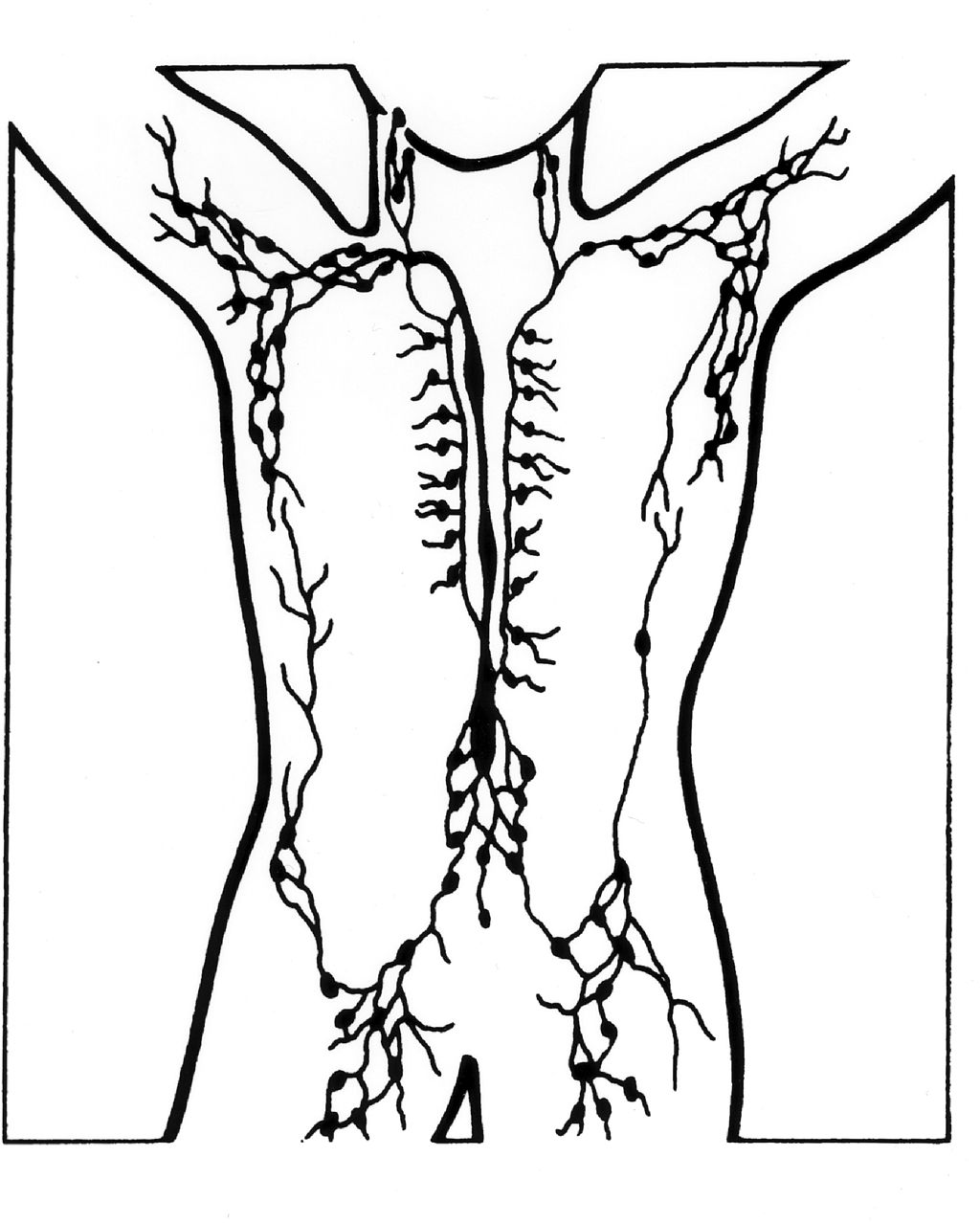
By Unknown Illustrator - This image was released by the National Cancer Institute, an agency part of the National Institutes of Health, with the ID 3237 (image) (next).This tag does not indicate the copyright status of the attached work. A normal copyright tag is still required. See Commons:Licensing for more information.English | Français | +/−, Public Domain, https://commons.wikimedia.org/w/index.php?curid=24052444
|
Leukemia
Common Symptoms of Leukemia:

Many Leukemias Affect White Blood Cells in the Bone Marrow:

White Blood Cells Infected With Leukemia (Lose Shape/Structure, Become Crowded):

Acute Lymphoblastic/Lymphocytic Leukemia (ALL):
Acute lymphocytic leukemia (ALL) is characterized by overproduction of immature cells of the lymphoid line called lymphoblasts found in the bone marrow and lymph nodes. ALL is the main type of leukemia to affect children, typically between the ages of 2-15 years of age. It also tends to affect those >65 years of age. Of all adult leukemias, this type accounts for 20%. With early diagnosis and treatment, prognosis is very good. If not recognized or treated, however, it can progress very quickly.
Risk factors for this type of leukemia include past chemotherapy for treatment of cancer, and some genetic conditions. Other risk factors may be exposure to X-rays and other forms of radiation before birth, prolonged exposure to certain chemicals or drugs, smoking, certain viruses, DNA mutations, changes or mutations in the chromosomes carrying genetic information, having Down Syndrome, having Fanconi anemia, having neurofibromatosis type 1, Bloom syndrome, or having Li-Fraumeni syndrome. There are 3 levels of risk:
With this type of leukemia, the bone marrow synthesizes too many lymphoblasts (immature lymphocytes), and they become crowded in the bone marrow, taking up >30% of it. It is a cancer of the blood and bone marrow. The cells are abnormal, mutated, and have irregular shapes and borders, irregular nuclei, and many times the cytoplasm becomes vacuolated (develops pockets or holes in it). In ALL, not only are the white blood cells affected, but the red blood cells and platelets can become affected as well. In this case, there are decreased numbers of erythrocytes and platelets. This means that the blood clotting can become affected, leading to easy bruising, and anemia can occur due to lack of iron and oxygen to the brain and body tissues. Frequent infections are common, because the white blood cells are the cells of immunity and if they are affected, it may result in decreased immunity to viruses, bacteria, fungi, and other microbes.
ALL is diagnosed by undergoing a thorough physical exam and history, and undergoing a complete blood count (CBC) with differential. Sometimes, CSF is withdrawn and analyzed as well. This blood test detects types and percentages of all blood cells and checks to see if they're in range, checks the oxygen being carried by the red blood cells and hemoglobin and iron levels. A blood chemistry is also analyzed to see if there are increases or decreases in various substances that may indicate disease. If these tests come back abnormal, a bone marrow aspiration and biopsy is necessary to look for signs of cancer. Pathologists, cytopathologists, hematologists and immunologists review blood slides to diagnose the cancer, stage it, and immunotype it and see if it is B-lymphocytes or T-lymphocytes affected (lymphoid line) or if the cells of the myeloid line are affected. If cancer is confirmed, a lumbar tap may be necessary to see if the cancer has spread to the brain and spinal cord. A chest X-ray is also taken to see if the cancer has spread to the chest wall or lungs.
Treatment involves aggressive chemotherapy. Often times, this treatment is administered for 2-3 years. Radiation therapy may also be required if the CNS is involved. Individuals with the Philadelphia chromosome are usually give drug therapy as well. Those who do not respond well to treatment may be candidates for bone marrow transplant.
Overall prognosis for 5-year survival rate is pretty promising with treatment at 78-85%. Children who are treated have a better prognosis than adults at time of diagnosis. Prognosis is based on a number of factors including:
Peripheral Blood: Expect to see
Bone Marrow:
Risk factors for this type of leukemia include past chemotherapy for treatment of cancer, and some genetic conditions. Other risk factors may be exposure to X-rays and other forms of radiation before birth, prolonged exposure to certain chemicals or drugs, smoking, certain viruses, DNA mutations, changes or mutations in the chromosomes carrying genetic information, having Down Syndrome, having Fanconi anemia, having neurofibromatosis type 1, Bloom syndrome, or having Li-Fraumeni syndrome. There are 3 levels of risk:
- Standard or low risk: Ages 1 to <10 years of age; WBC count <50,000/uL at time of diagnosis
- High risk: >10 years of age; WBC >50,000/uL at time of diagnosis
- Very high risk: <1 year of age; changes in a gene or genes; slow initial response to treatment; not responding after 4 weeks of treatment
With this type of leukemia, the bone marrow synthesizes too many lymphoblasts (immature lymphocytes), and they become crowded in the bone marrow, taking up >30% of it. It is a cancer of the blood and bone marrow. The cells are abnormal, mutated, and have irregular shapes and borders, irregular nuclei, and many times the cytoplasm becomes vacuolated (develops pockets or holes in it). In ALL, not only are the white blood cells affected, but the red blood cells and platelets can become affected as well. In this case, there are decreased numbers of erythrocytes and platelets. This means that the blood clotting can become affected, leading to easy bruising, and anemia can occur due to lack of iron and oxygen to the brain and body tissues. Frequent infections are common, because the white blood cells are the cells of immunity and if they are affected, it may result in decreased immunity to viruses, bacteria, fungi, and other microbes.
ALL is diagnosed by undergoing a thorough physical exam and history, and undergoing a complete blood count (CBC) with differential. Sometimes, CSF is withdrawn and analyzed as well. This blood test detects types and percentages of all blood cells and checks to see if they're in range, checks the oxygen being carried by the red blood cells and hemoglobin and iron levels. A blood chemistry is also analyzed to see if there are increases or decreases in various substances that may indicate disease. If these tests come back abnormal, a bone marrow aspiration and biopsy is necessary to look for signs of cancer. Pathologists, cytopathologists, hematologists and immunologists review blood slides to diagnose the cancer, stage it, and immunotype it and see if it is B-lymphocytes or T-lymphocytes affected (lymphoid line) or if the cells of the myeloid line are affected. If cancer is confirmed, a lumbar tap may be necessary to see if the cancer has spread to the brain and spinal cord. A chest X-ray is also taken to see if the cancer has spread to the chest wall or lungs.
Treatment involves aggressive chemotherapy. Often times, this treatment is administered for 2-3 years. Radiation therapy may also be required if the CNS is involved. Individuals with the Philadelphia chromosome are usually give drug therapy as well. Those who do not respond well to treatment may be candidates for bone marrow transplant.
Overall prognosis for 5-year survival rate is pretty promising with treatment at 78-85%. Children who are treated have a better prognosis than adults at time of diagnosis. Prognosis is based on a number of factors including:
- Age at diagnosis
- Gender
- Race
- Ethnicity
- Number of white blood cells in the peripheral bloodstream at the time of diagnosis
- If the leukemia is affecting B- or T-lymphocytes
- If there are any chromosomes that are associated with the cancer, such as the Philadelphia chromosome
- If there are underlying genetic disorders or other illnesses
- If the cancer cells have spread to the CSF, brain or spinal cord or other parts of the body
- Weight at diagnosis and treatment
- How well treatment works and if the cells respond to treatment
- If there is a relapse
Peripheral Blood: Expect to see
- blasts, small blasts (1-2.5 the size of a resting lymphocyte) or large blasts (2-3x the size of a resting lymphocyte)
- scant blue cytoplasm to moderate cytoplasm
- condensed chromatin
- irregular nuclear membrane
- indistinct nucleoli or prominent if large blast
- thrombocytopenia
Bone Marrow:
- >20% of all nucleated cells make up a homogenous population of blasts
Gallery of Slides of ALL:

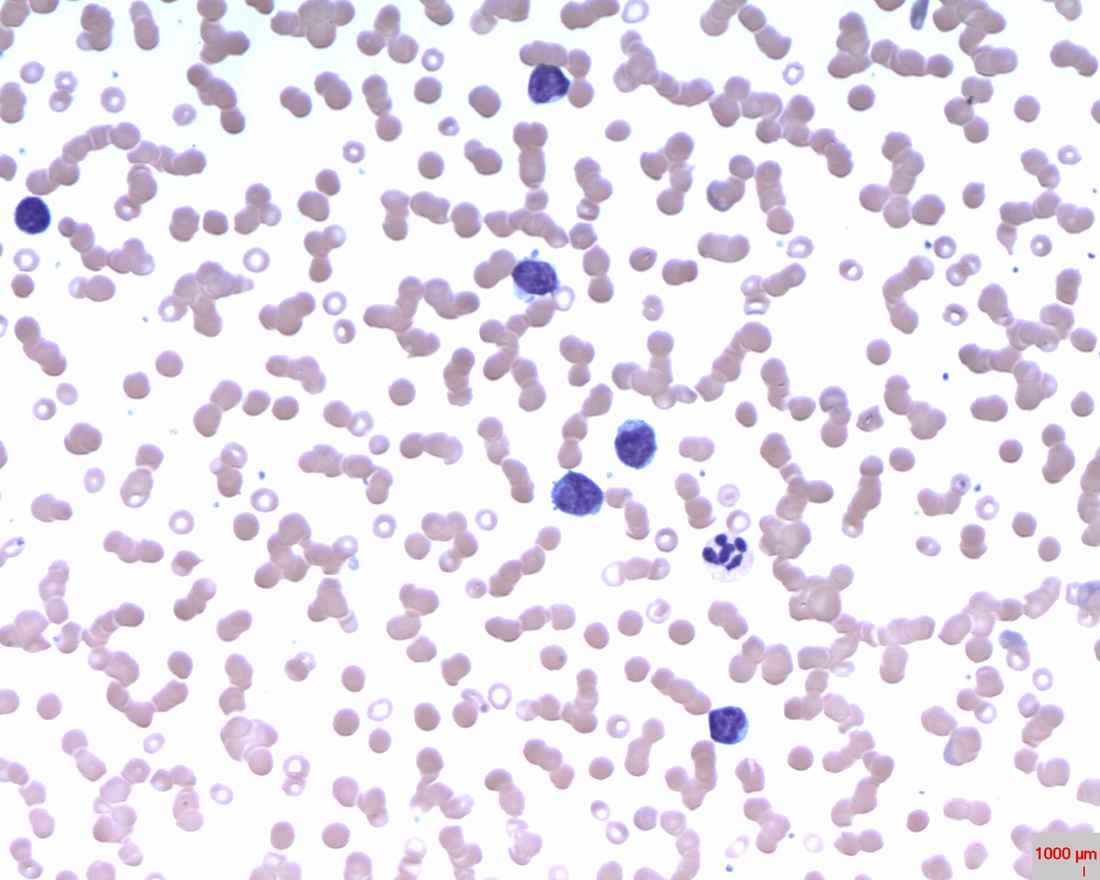
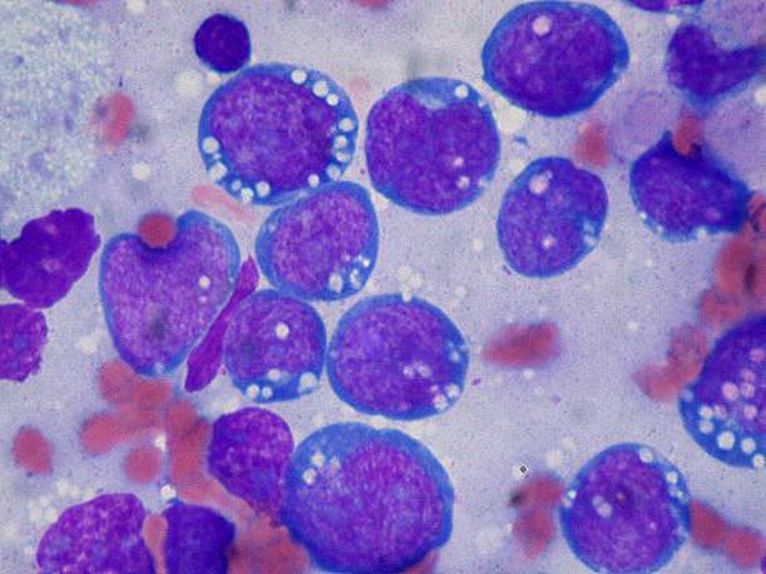
Lymphoblasts infiltrating the peripheral bloodstream in this smear of ALL...Normally, lymphoblasts are only seen in the bone marrow, however, if seen in the peripheral smear, this is a sign of blast crisis and leukemia is suspected. Notice how the lymphoblasts are misshapen, full of vacuoles, and the cytoplasm is irregular in ALL.

ALL Fab L1: +/- blasts, small blasts with scant blue cytoplasm; round nucleoli; some vacuoles; thrombocytopenia)

ALL Fab L2: Blasts 2-3x the size of a resting lymphocyte, moderate cytoplasm, the nuclear membrane is irregular, nucleoli; thrombocytopenia)

ALL Fab L3: Blast crisis, with overcrowding of irregular lymphoblasts in the bone marrow; These blasts are large with dark blue cytoplasm, many vacuoles in the cytoplasm, 3-5 nucleoli, and thrombocytopenia
Acute Myelogenous/Myeloid Leukemia (AML)
Acute Myeloid Leukemia (AML) is a type of leukemia that affects the myeloid cell line (myeloblasts, or immature myelocytes) in the bone marrow. It can also affect the red blood cells and platelets. AML is the umbrella term, but there are various subtypes of this leukemia. This type of leukemia tends to be aggressive and rapidly progressive if not diagnosed and treated quickly, and it is the most common type of acute leukemia to affect adults. Of all childhood leukemias, this one accounts for about 20%. About 10-15% of cases are caused by prior treatment with chemotherapy or radiation for other types of cancers.
With AML, there is a rapid buildup of myeloblasts of the myeloid line in the bone marrow, which spill over into the peripheral blood and other tissues. This leads to pancytopenia and a multitude of symptoms.
This type of leukemia mainly affects those in middle age (30-50), however, it can affect all ages. Symptoms begin abruptly and intensely. It results in the malignant, unregulated proliferation of myeloid progenitor cells (immature cells). Untreated, it leads to death within months of diagnosis (as little as 2-3 months), resulting in hemorrhage and infection. A type of anemia is common (normocytic-normochromic) with a decrease in red blood cells, platelets, and an increase in leukocytes with >60% blasts seen in the peripheral blood smear (no blasts should ever be seen here). Treatment includes chemotherapy, a possible transfusion, and a bone marrow transplant.
Risk factors include:
Treatment is 2 stages and includes 4 things: radiation, chemotherapy, stem cell transplant, and other drugs over a 21-month period.
Prognosis is also based on the same factors as seen in ALL. Overall 5-year survival rate ranges from 15-70% with treatment.
Peripheral Blood Slide:
With AML, there is a rapid buildup of myeloblasts of the myeloid line in the bone marrow, which spill over into the peripheral blood and other tissues. This leads to pancytopenia and a multitude of symptoms.
This type of leukemia mainly affects those in middle age (30-50), however, it can affect all ages. Symptoms begin abruptly and intensely. It results in the malignant, unregulated proliferation of myeloid progenitor cells (immature cells). Untreated, it leads to death within months of diagnosis (as little as 2-3 months), resulting in hemorrhage and infection. A type of anemia is common (normocytic-normochromic) with a decrease in red blood cells, platelets, and an increase in leukocytes with >60% blasts seen in the peripheral blood smear (no blasts should ever be seen here). Treatment includes chemotherapy, a possible transfusion, and a bone marrow transplant.
Risk factors include:
- Smoking
- Relative with AML
- Exposure to ionizing radiation or X-rays
- Prior chemotherapy
- Males are at higher risk
- >60 years of age are at higher risk
- Had ALL as a child and had treatment for it
- Exposure to the chemical benzene in gasoline, rubber cement, and other cleaning solvents)
- Fevers
- Fatigue
- Easy bruising
- Easy bleeding (gums, mucous membranes)
- Shortness of breath
- Weakness
- Weight loss
- Loss of appetite
- Infections
Treatment is 2 stages and includes 4 things: radiation, chemotherapy, stem cell transplant, and other drugs over a 21-month period.
Prognosis is also based on the same factors as seen in ALL. Overall 5-year survival rate ranges from 15-70% with treatment.
Peripheral Blood Slide:
- Large, irregular blasts, agranular
- Possible Auer rods in the myeloblasts
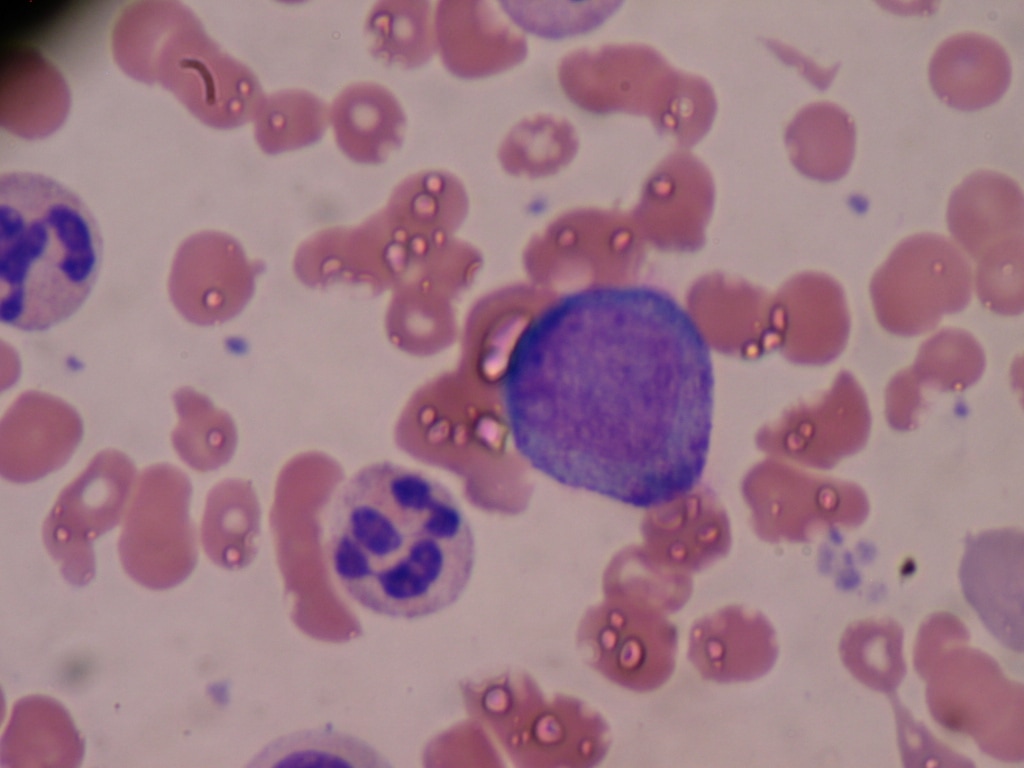
Gallery of Slide Images of AML:


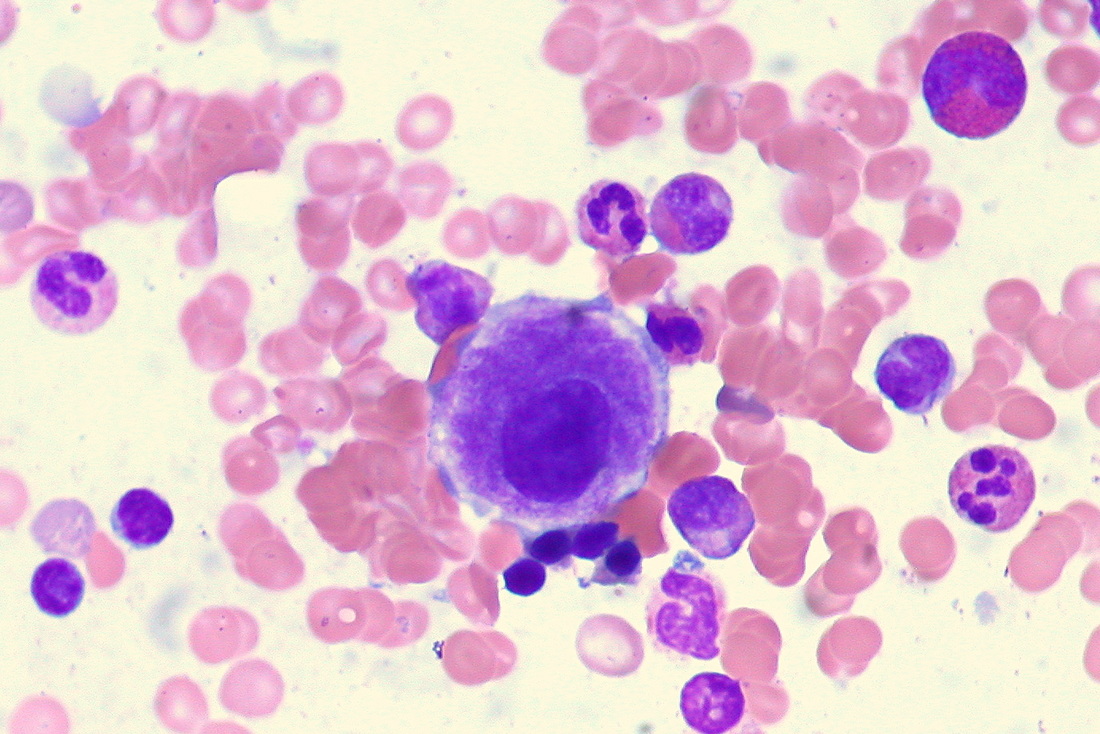
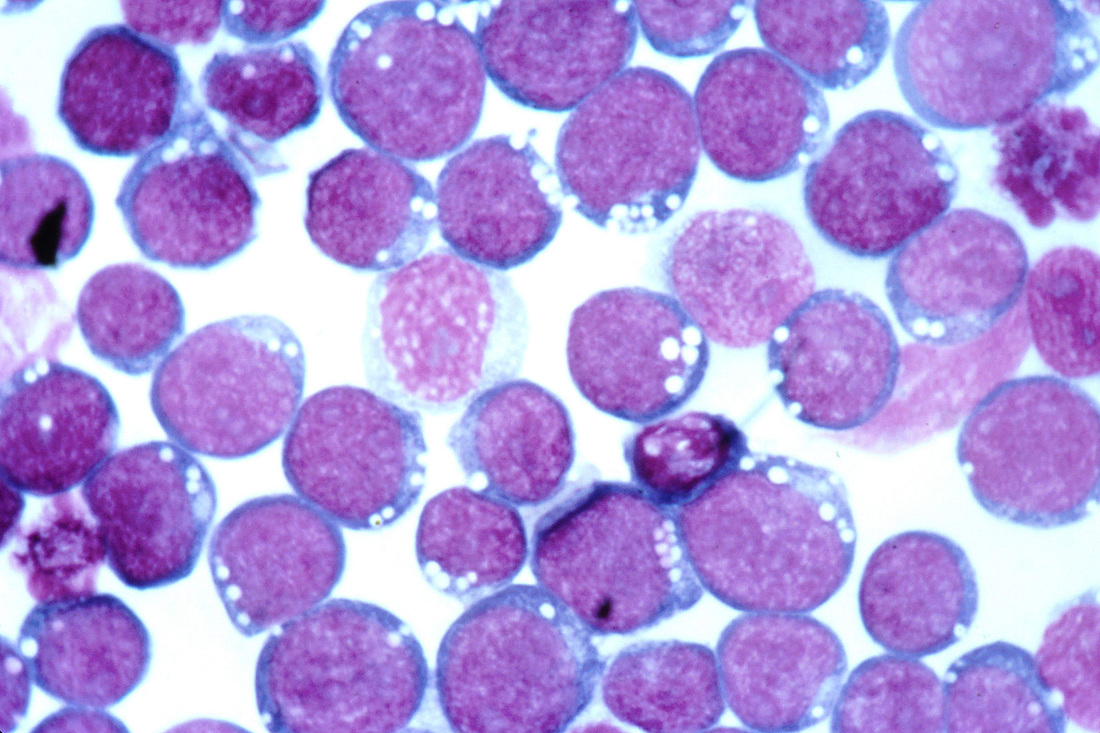
In AML, irregular monoblasts are seen in the peripheral bloodstream (normally monoblasts are only seen in the bone marrow)

Blast crisis: numerous monoblasts in peripheral bloodstream (notice the irregularity of the shape, cytoplasm, and the presence of vacuoles) (large, agranular blasts and thrombocytopenia)

AML (M1) without maturation (blasts, thrombocytopenia in peripheral blood)

AML (M2) with maturation and differentiation (blasts with some maturation, +/- Auer rods, thrombocytopenia in peripheral blood)

AML (M2) with maturation, characteristic Auer rods, granulation, and vacuolization, several blasts with prominent nucleoli, a myelocyte and a promyelocyte

AML (M3) Hypergranular Acute Promyelocytic Leukemia. Cells are displaying an overabundance of azurophilic granules, bilobed or kidney-shaped nuclei, multiple Auer rods are possible and may be in bundles); MPO/SBB---strongly positive (+)

AML (M3-V) Acute Promyelocytic Leukemia, Microgranular Variant (abnormal promyelocytes varying in size) (Deeply notched nuclei; granules not visible in typical light microscopy; MPO-SBB---strongly positive)

AML (M4) Acute Myelomonocytic Leukemia (myeloblasts and other immature myeloid cells are seen in the peripheral blood, along with monocytoid cells, +/- Auer rods, and thrombocytopenia)

AML (M4EO) Acute Myelomonocytic Leukemia With Increased Marrow Eosinophils (In the peripheral blood, myeloblasts and other immature myeloid cells are seen, along with monocytoid cells and thrombocytopenia)

AML (M5) Acute Monoblastic or Monocytic Leukemia, Poorly Differentiated, 5a) (blasts and thrombocytopenia in peripheral blood; NBE-positive)
AML (M5B) Acute Monocytic Leukemia bone marrow smear (notice the folds and creases of the cytoplasm in the monocytes) (blasts, monocytoid cells, thrombocytopenia, NBE-positive, well-differentiated)

AML (M6) Erythroleukemia in peripheral blood smear in asplenic patient (thrombocytopenia, dimorphic, dichromic erythroid population, basophilic stippling, nucleated erythrocytes, +/- blasts)


Auer rods in bone marrow aspirate of patient with AML
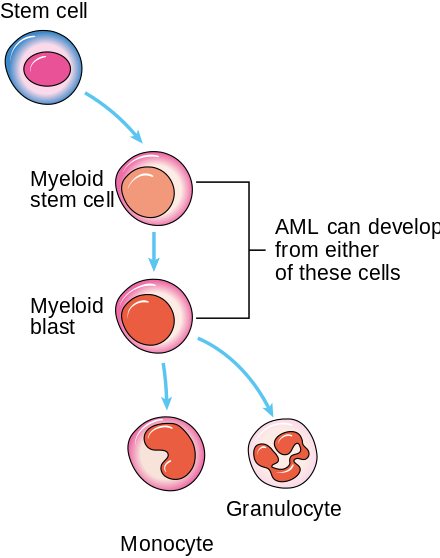
Development of AML

Numerous Auer rods and Pelger Huet cells commonly seen in this type (AML, M3, Promyelocytic AML)

Acute Promyelocytic Leukemia (APL):
APL is a type of AML that is characterized by a translocation between the long arms of chromosomes 15 and 17, which creates a fusion gene. This gene impairs differentiation and apoptosis of promyelocytes. Administration of all-trans retinoic acid, a derivative of vitamin A, is desired and is often used in conjunction with chemotherapy.
Peripheral Blood Smear:
Peripheral Blood Smear:
- WBC may be low or only slightly elevated
- Blasts
- Hypergranular promyelocytes
- Gray or blue cytoplasm
- Nucleus may be folded or bilobed or deeply notched
- Multiple Auer rods, possibly in bundles
- Schistocytes (RBC's: helmet cells, fragments)
Neutrophilic promyelocyte; CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=1249872
|

Eosinophilic promyelocyte; CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=1249856
|

Basophilic promyelocyte;CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=1249847
|
Promyelocyte in bone marrow; By Bobjgalindo - Own work, GFDL, https://commons.wikimedia.org/w/index.php?curid=7777605
Chronic Myelogenous/Myelocytic Leukemia (CML)
Chronic Myelogenous Leukemia (CML) is a slow-growing cancer of the blood and bone marrow that worsens over time. The bone marrow produces too many granulocytes. Typically, there is an excess of mature neutrophils, which have decreased function. It accounts for about 15-20% of all leukemias in adults. There are 3 phases:
Risk Factors:
Prognosis:
Treatment:
- Chronic phase: <10% of the cells in the blood and bone marrow are blasts
- Accelerated phase: 10-19% of the cells in the blood and bone marrow are blasts
- Blast phase: 20% of the cells in the blood and bone marrow are blasts (blast crisis)
- Tiredness
- Fever
- Enlarged and tender spleen
- Fevers
- Night Sweats
- Fatigue
- Weight loss
- Bleeding
- Pain and a feeling of fullness below the ribs, especially in the upper left quadrant
- Acute, gouty arthritis
- Tenderness in the lower sternum
- Anemia
- Splenomegaly
Risk Factors:
- Gene mutations
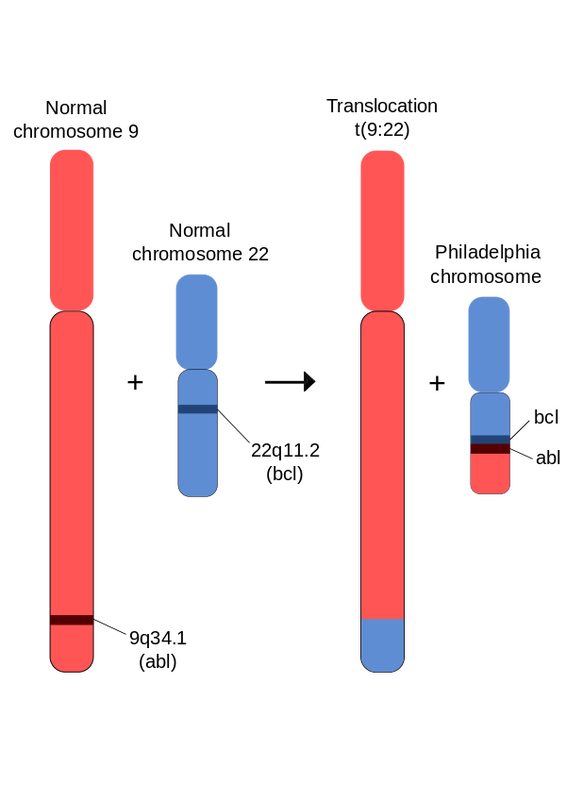
- Philadelphia chromosome (chromosome 22)
- >40 years of age
- Exposure to ionizing radiation
Prognosis:
- Similar factors as ALL and AML
- Depends on remission or relapse as well
- Overall 5-year survival rate is just 35%
Treatment:
- Bone marrow transplant is the only known treatment for complete cure (only an option for about 25% of individuals)
- Drug that inhibits Bcr/Abl tyrosine kinase
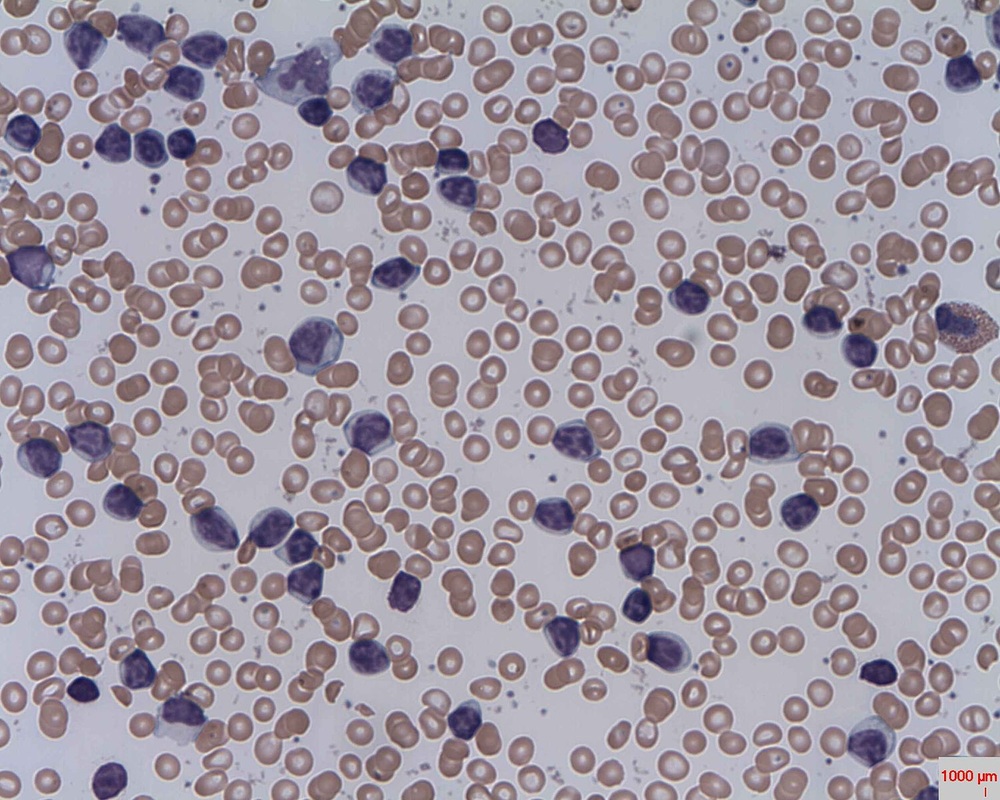
Gallery of Slide Images of CML:

Many Pelger Huet Neutrophils (abnormal) are seen here along with other affected granulocytes
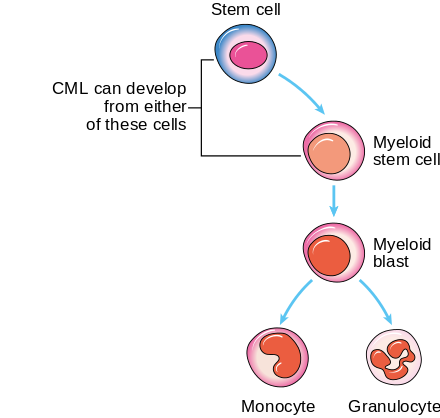
Development of CML
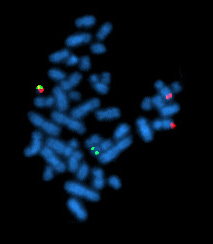
This type is associated with the Philadelphia chromosome
|
|


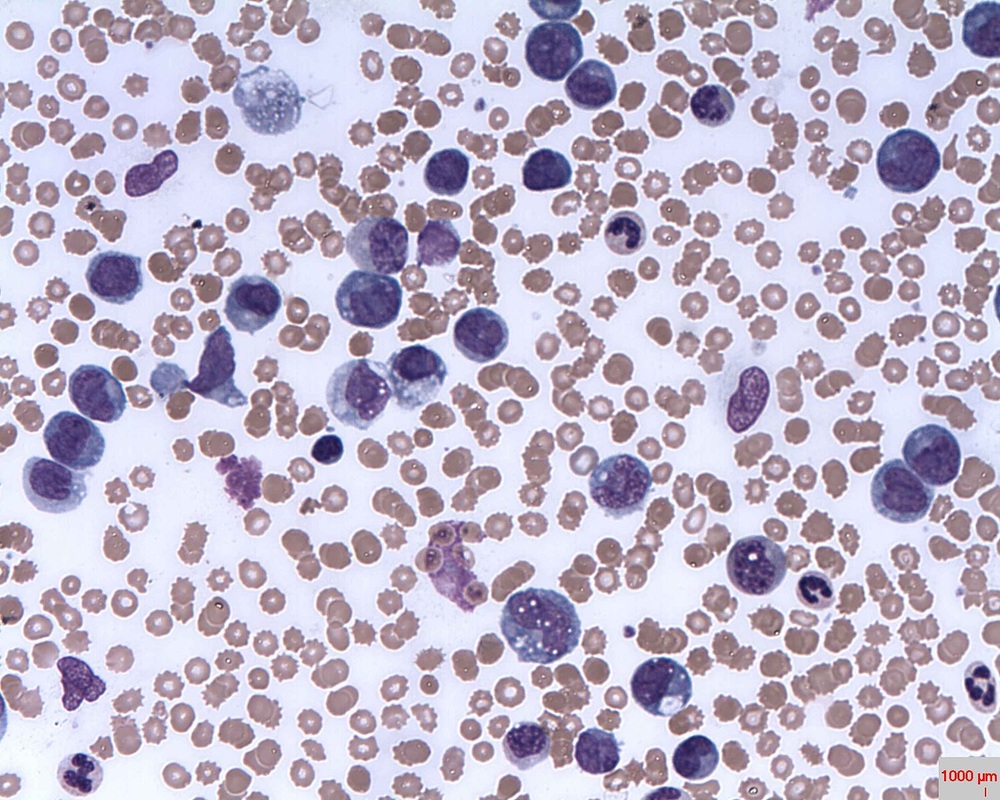
Peripheral Blood Slide:
- WBC increased
- RBC normal or decreased
- Platelets normal or decreased
- Myeloblasts
- Pseudo-Pelger-Huet cells
- Basophilia
- Eosinophilia
- Monocytosis
Chronic Lymphocytic Leukemia (CLL)
Chronic Lymphocytic Leukemia (CLL) is a leukemia that affects the B-lymphocytes, WBCs of the immune system that secrete antibodies. Is slowly progressive and causes the buildup of mature but dysfunctional lymphocytes in the bone marrow. At first, individuals may be asymptomatic, but a routine CBC may reveal the following: lymphocytosis, thrombocytopenia, anemia.
There are 5 stages of the disease (Rai system), and overall survival rate ranges from 2-20 years, where overall 5-year survival rate is 78% with treatment:
Symptoms:
Treatment:
Peripheral Blood Slide:
There are 5 stages of the disease (Rai system), and overall survival rate ranges from 2-20 years, where overall 5-year survival rate is 78% with treatment:
- Stage 0: lymphocytosis and bone marrow infiltration of >30% blasts; Median survival: 12 years
- Stage 1: lymphadenopathy; Median survival: 9 years
- Stage 2: splenomegaly; Median survival: 6 years
- Stage 3: anemia; Median survival: 1 year
- Stage 4: thrombocytopenia; Median survival: 1 year
Symptoms:
- Painless, swollen lymph nodes
- Fatigue
- Pain and fullness below the ribs
- Fever
- Night sweats
- Frequent viral and fungal infections
- Weight loss
Treatment:
- Withheld unless patient is symptomatic and has hemolytic anemia, painful lymphadenopathy, splenomegaly, prolonged fever, chills, weight loss
- Chemotherapy
- Raiation therapy
- Drug therapy
- Bone marrow transplant is usually not an option
Peripheral Blood Slide:
- Small lymphocytes
- Smudge cells
- Thrombocytopenia
Gallery of Slide Images of CLL:

B-Cell CLL bone marrow smear
Smudge cells of CLL in peripheral blood

Smudge cells, common in CLL, are seen here in the peripheral blood

CLL with autoimmune hemolytic anemia

Development of CLL

Affected B cells

Affected B cells with "turtle shell" appearing cytoplasm
Hairy Cell Leukemia:
This rare leukemia of B-lymphocytes is a chronic, slow-growing cancer that causes the B-lymphocyte cytoplasm to appear "hairy" or "ruffled". Hairy cell leukemia is considered to be one of the chronic lymphoproliferative disorders. The most common age group affected are men in their middle age to elderly. It accounts for just 2-5% of all cases of leukemia. The spleen, liver and bone marrow are affected and sometimes the lymph nodes are affected as well.
Risk Factors:
Symptoms may include the following:
Peripheral blood smear:
Risk Factors:
- Being male
- Middle-age or older
- Mutations in DNA
- Exposure to radiation
- Exposure to carcinogens in chemicals
- Exposure to sawdust
- Those of Ashkenazi Jewish heritage are at higher risk for infection
Symptoms may include the following:
- A feeling of fullness in the abdomen due to splenomegaly
- Loss of appetite or feeling full very quickly
- Weakness and fatigue
- Bruising easily
- Infections
- Unintentional weight loss
- Anemia
- Bruising or bleeding from mucous membranes
- Onset of other types of cancers such as non-Hodgkin's lymphoma
Peripheral blood smear:
- small or medium round to ovoid lymphocytes with diffuse homogenous chromatin
- nuclei is typically oval or indented
- nucleolus may or may not be present
- irregular cytoplasm
- Gray-blue hairlike projections
- pancytopenia
- reactive lymphocytes
- vacuoles may be possible
- RBCs may be clumped or display some rouleaux

The cytoplasm in Hairy Cell Leukemia is unique in that it looks "hairy" and ruffled in appearance (abnormal B cells)

This is a nice close-up image of several hairy cells characteristic of hairy cell leukemia

Hairy cell leukemia is a sub-type of CLL and this slide has numerous hairy cell lymphocytes
6 ruffled lymphocytes are seen in this slide of an individual with hairy cell leukemia
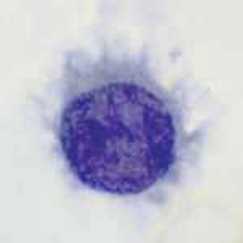
A great close-up view of the cytoplasmic streaming forming "hairlike" structures that are characteristic of hairy cell leukemia
Multiple Myeloma (MM)
This type of cancer is serious because it affects B-lymphocytes that secrete antibodies (plasma cells). Without this type of immunity, an individual is at risk for serious and recurring infections without the ability to fight them off. Tumors called plasmacytomas may form in places in the body such as the bone.
Symptoms may include:
Symptoms may include:
- Anemia
- Low blood counts
- High blood calcium
- Infections
- Kidney problems
- Amyloidosis

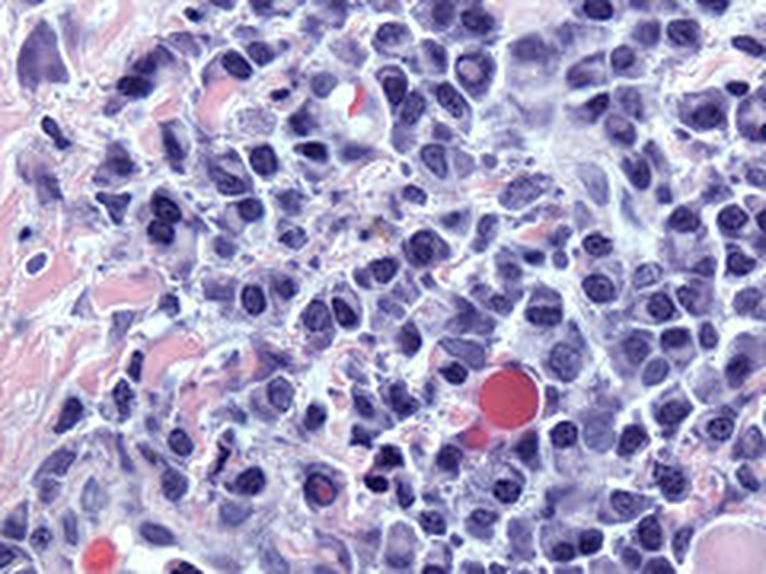
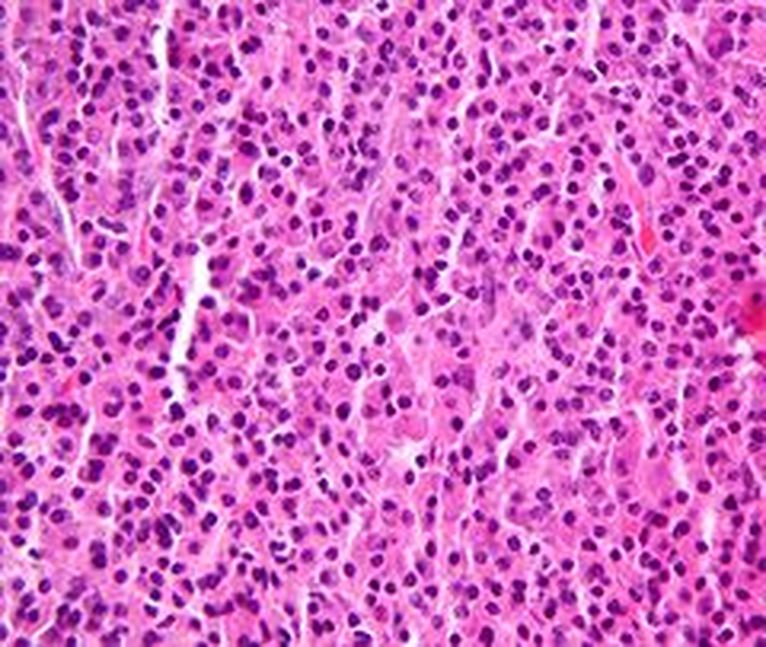
Multiple myeloma in bone marrow smear

Multiple myeloma in bone marrow aspirate prepared smear

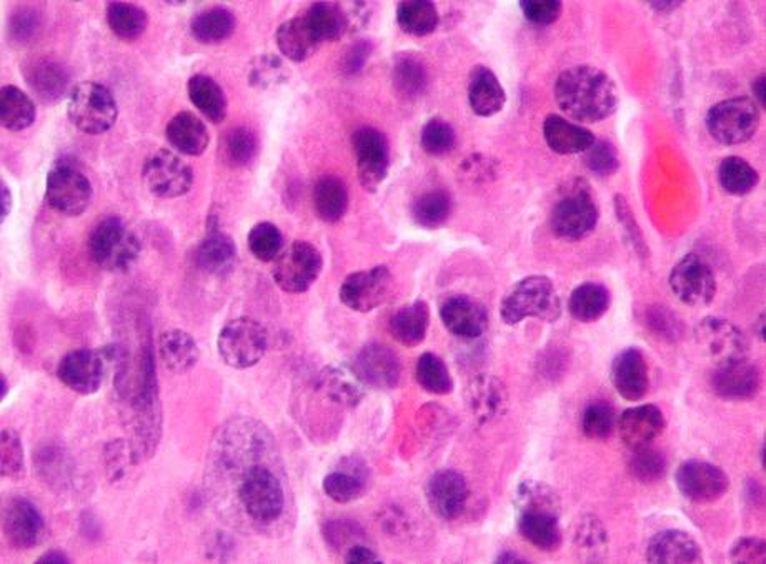
Plasma cells in multiple myeloma (MM)

Mott Cell-Plasma cell with spherical inclusions in the cytoplasm

Flame cells, malignant plasma cells and Russell Bodies

Malignant plasma cells, Mott cell and Russell bodies

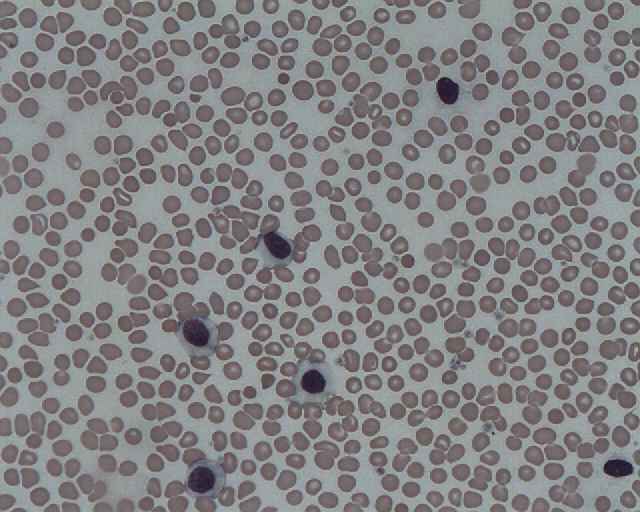
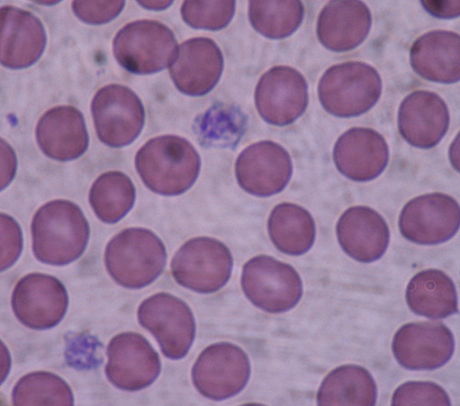
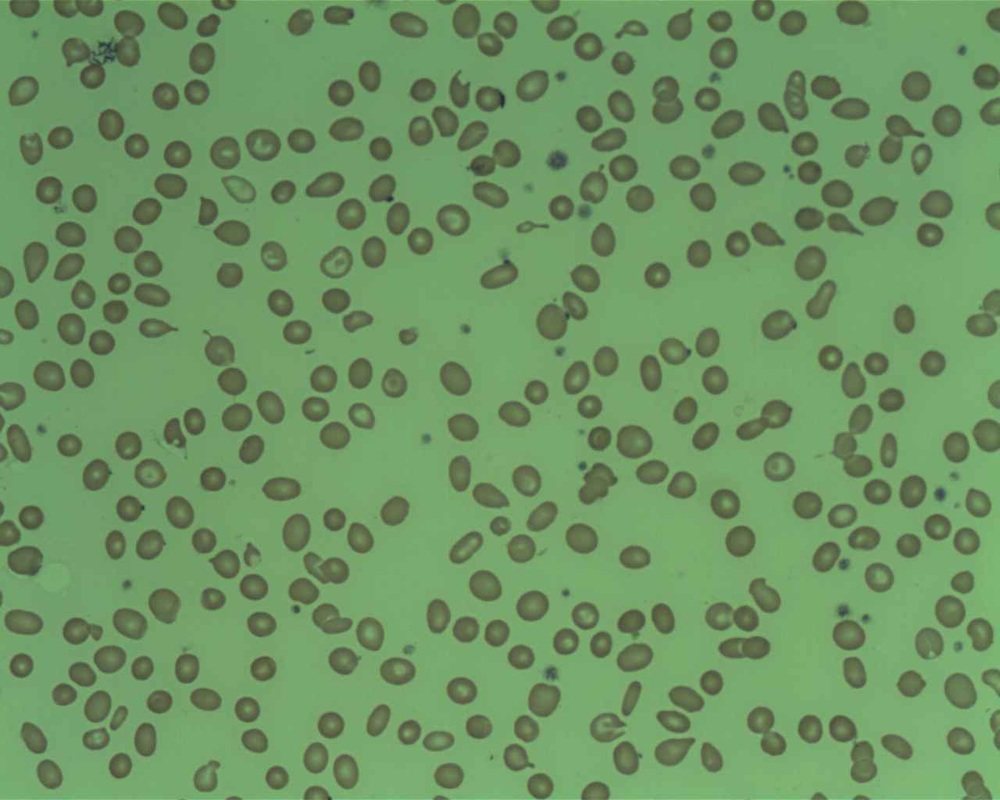
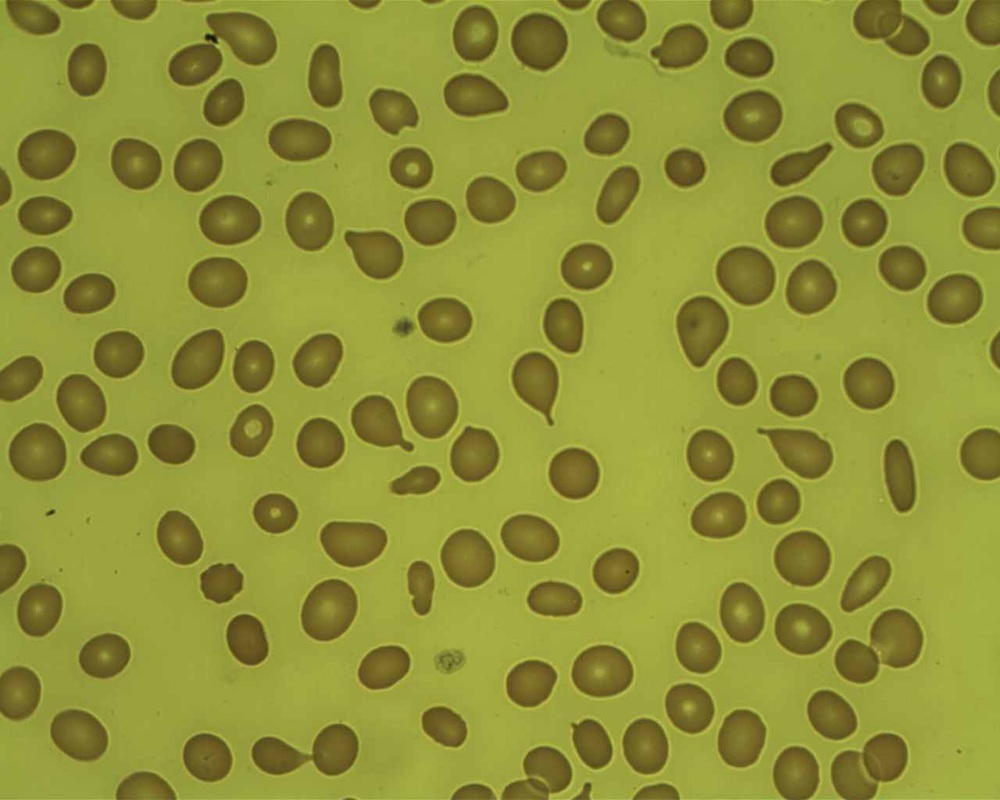
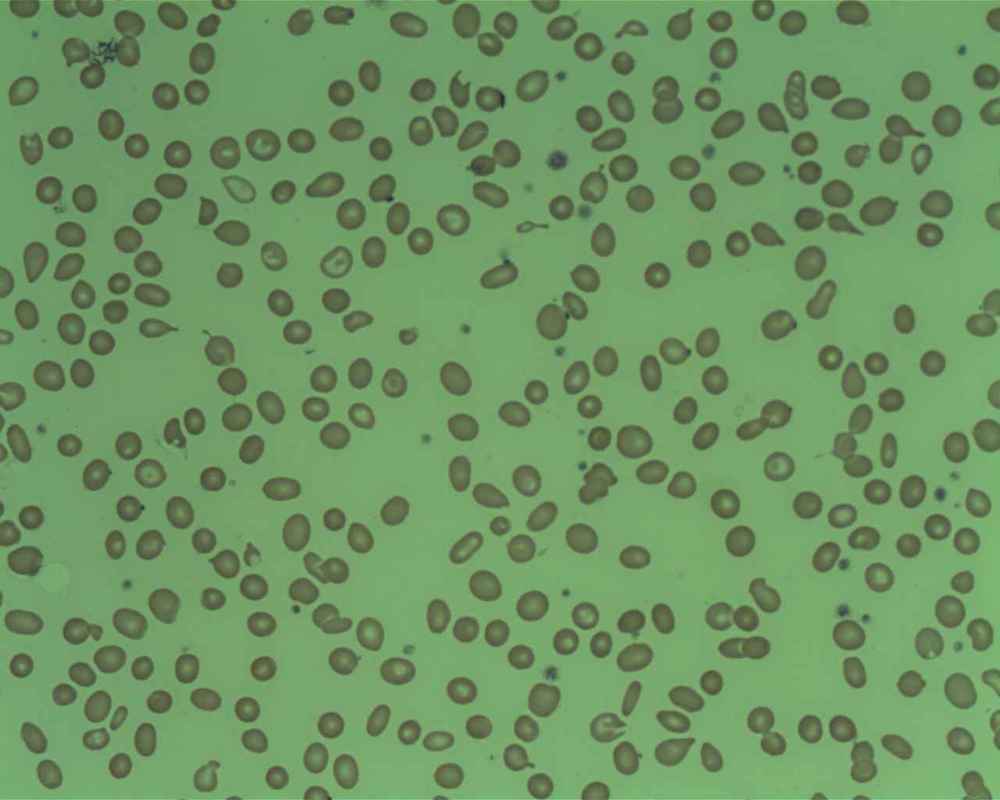
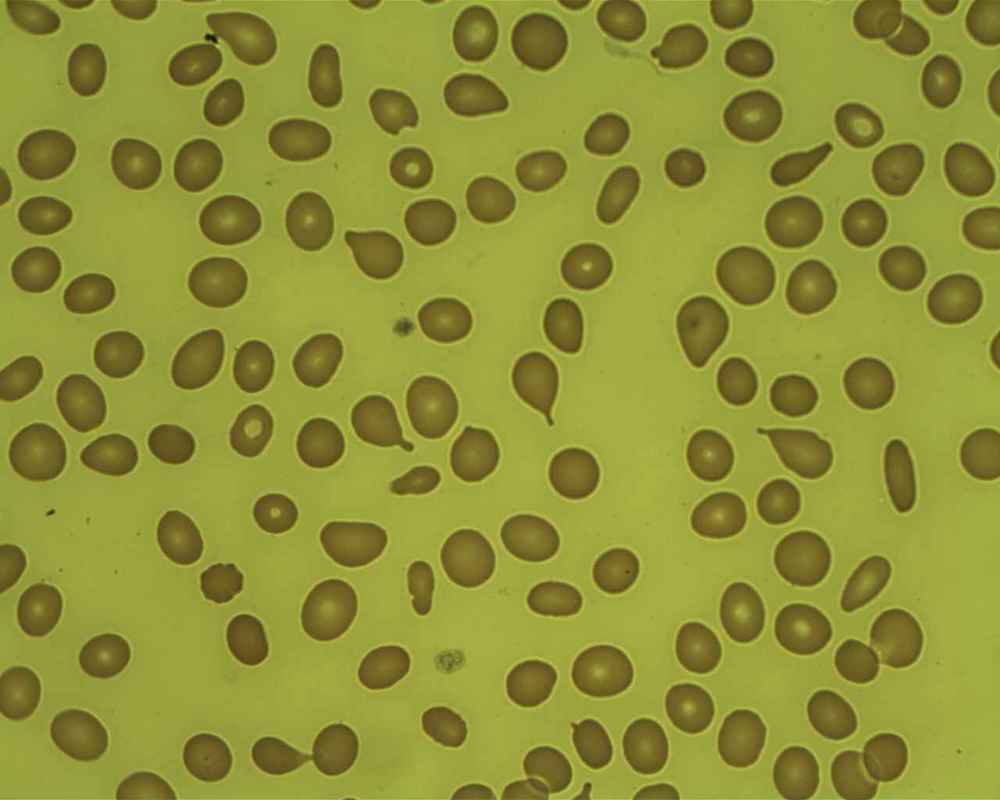
Affected lymphocytes; rouleaux (stacked coin appearance) of red blood cells is commonly seen with MM
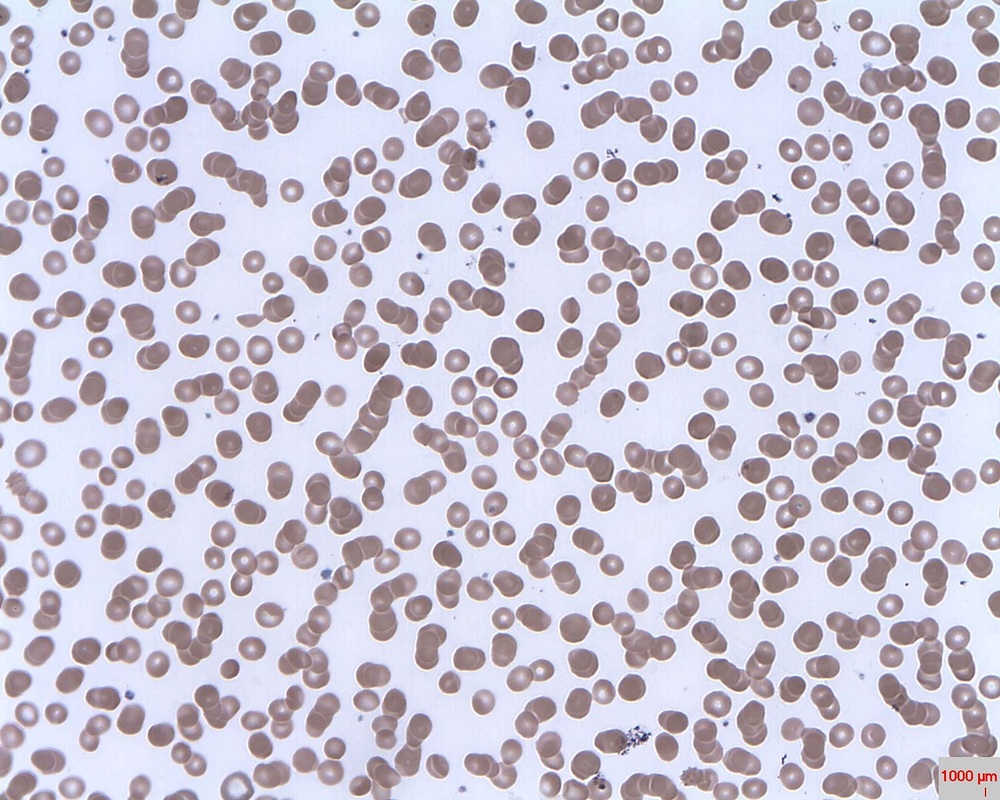
Rouleaux is commonly seen
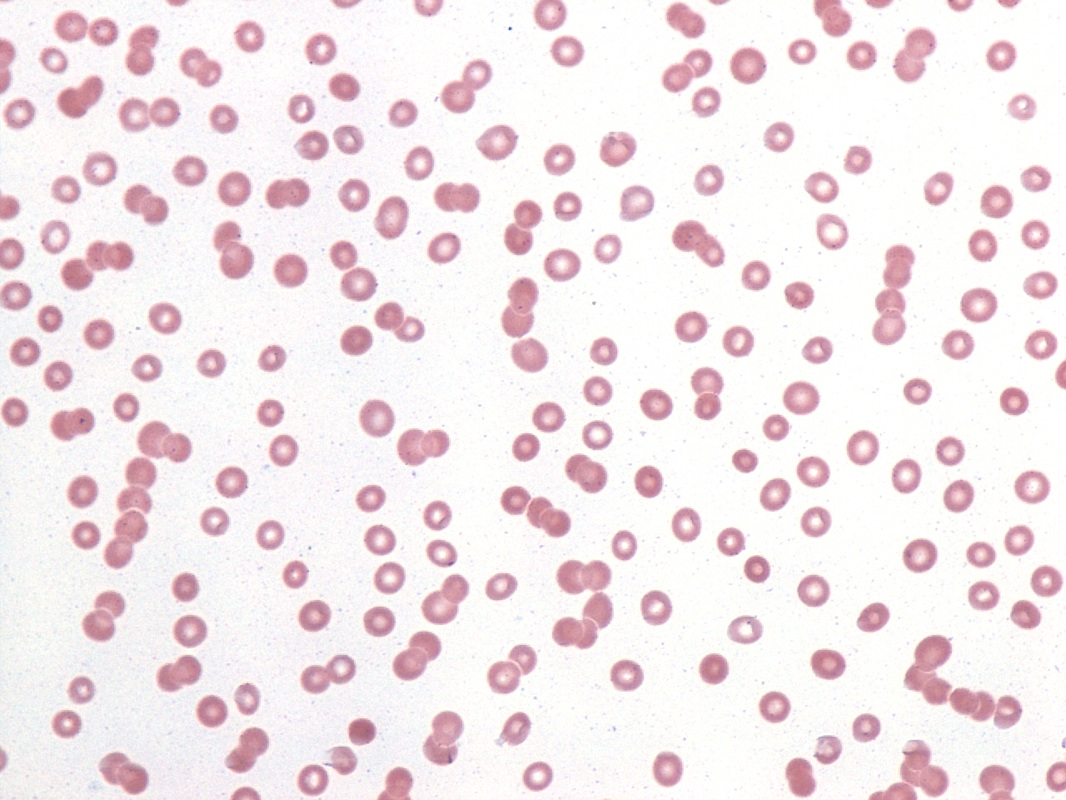
Rouleaux is commonly seen with this disease

B lymphocytes are affected here and the dysplastic cells reveal increased vacuolization
Russell bodies and flame cells
Russell bodies and flame cells
Lymphomas:
Lymphomas are malignant neoplasms of the cellular components of the lymphatic system. The affected cells may be B cells, T cells or, rarely, both. They may travel to other areas of the body, including the bloodstream, bone marrow, and even non-lymph organs such as the liver or lungs. There are 2 main categories of lymphomas:
- Hodgkin's disease
- Other types, grouped as non-Hodgkin's disease
- Stage 1: one single lymph node structure OR region is involved
- Stage 2: two or more lymph nodes or structures are involved, and both are on the same side of the diaphragm
- Stage 3: the lymph regions on BOTH sides of the diaphragm are involved
- Stage 4: there is widespread involvement of extranodal tissue both above AND below the diaphragm
Hodgkin's Lymphoma
Hodgkin's disease, or Hodgkin's lymphoma, is a type of malignant cancer that starts in the white blood cells (lymphocytes) in the body's lymphatic system. It represents about 15% of all lymphomas. Tumors arise in the lymph node tissue then spread to other lymph nodes, the spleen, the liver and bone marrow.
The disease was named after its discoverer: Dr. Thomas Hodgkin. Hodgkin's lymphoma affects the lymphatic system: the lymph nodes, lymphoid tissue in other areas of the body, including the thymus gland and Peyer's patches in the intestine, the tonsils, the adenoids, the spleen, the gut (colon, stomach, intestines, rectum), the bone marrow, the lymph, and the lymphatic vessels and capillaries. Since these tissues are so widespread, this type of cancer can start just about anywhere, so symptoms depend upon which area the cancer has affected.
Most of the time, the cancer starts in the lymph nodes of the upper body. The neck, armpits, and chest are the most common lymph nodes affected first, and they are usually swollen, hard, and painless. At first, the disease spreads slowly from lymph node to lymph node, but in later stages, it can become more widespread and affect the bloodstream, liver, lungs, and even the bone marrow. There are two main types of Hodgkin lymphoma, and they are classified based on their microscopic appearance:
Symptoms commonly include:
Risk factors include:
Treatment:
Prognosis:
The disease was named after its discoverer: Dr. Thomas Hodgkin. Hodgkin's lymphoma affects the lymphatic system: the lymph nodes, lymphoid tissue in other areas of the body, including the thymus gland and Peyer's patches in the intestine, the tonsils, the adenoids, the spleen, the gut (colon, stomach, intestines, rectum), the bone marrow, the lymph, and the lymphatic vessels and capillaries. Since these tissues are so widespread, this type of cancer can start just about anywhere, so symptoms depend upon which area the cancer has affected.
Most of the time, the cancer starts in the lymph nodes of the upper body. The neck, armpits, and chest are the most common lymph nodes affected first, and they are usually swollen, hard, and painless. At first, the disease spreads slowly from lymph node to lymph node, but in later stages, it can become more widespread and affect the bloodstream, liver, lungs, and even the bone marrow. There are two main types of Hodgkin lymphoma, and they are classified based on their microscopic appearance:
- Classic Hodgkin Disease and its Subtypes (95% of cases)
- Recognized by distinct cells called "Reed-Sternberg" cells (an abnormal B-lymphocyte) (See image below)
- Subtype 1: Nodular Sclerosis (60-80% of cases; usually begins in chest or neck)
- Teens or young adults usually affected
- Subtype 2: Mixed Cellularity (15-30%; usually begins in upper body but can start in any lymph node)
- Older adults usually affected
- Subtype 3: Lymphocyte-Rich (5%; usually found in upper body and only affects a few nodes)
- Subtype 4: Lymphocyte-Depleted (<1%; least common type)
- Usually affects older individuals
- Usually advanced when found
- Abdomen, liver, spleen and/or bone marrow typically affected
- Nodular Lymphocyte Predominant Hodgkin Disease (5% of cases)
- Recognized by distinct cells called "Popcorn cells" since they resemble popcorn microscopically and are variants of the Reed-Sternberg cells
- Usually begins in lymph nodes in the neck and armpit
- More common in men than women
Symptoms commonly include:
- Fevers
- Night sweats
- Weight loss
- Itchy skin
- Fatigue
- Loss of appetite
- Painless swollen lymph nodes in the neck or mediastinum
- Pain behind the breastbone
- Shortness of breath
- Alcohol-induced pain
Risk factors include:
- Age (in your 20's or >50 years of age)
- Previous cancer
- Prior treatment with chemotherapy or radiation
- Family history of Hodgkin's disease
- Other lymphomas
- Immunosuppression
- Exposure to the Epstein-Barr virus (infectious mononucleosis or "mono")
Treatment:
- Radiation therapy alone or in combination with chemotherapy
- Chemotherapy alone
- Relapses are treated with chemotherapy
- Multiple relapses are treated with bone marrow transplant
Prognosis:
- Prognosis is good because Hodgkin's lymphoma is one of the most treatable forms of cancer
- Overall 5-year survival rate: 90%
Gallery of Slide Images of Hodgkin's Lymphoma:

Popcorn cell

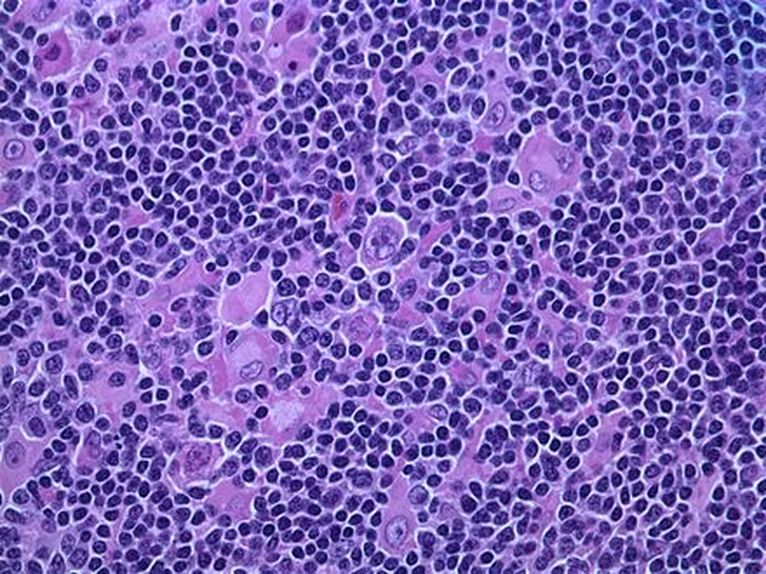
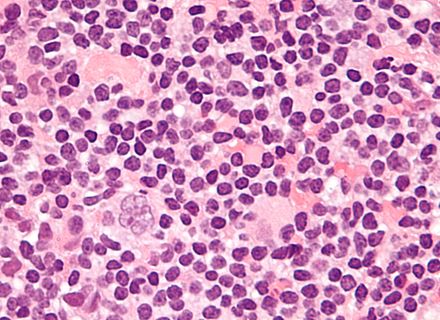
Reed-Sternberg cells


Reed-Sternberg cells, characteristic of Hodgkin's Lymphoma
Non-Hodgkin's Lymphoma
Non-Hodgkin's lymphomas also begin in the lymphocytes (white blood cells) in lymph nodes or tissues of the body. They can also be found on the bone. Both B- and/or T-lymphocytes can develop lymphoma, however, B-lymphocyte lymphomas are much more common in the USA. In fact, 90% of NHL's are from abnormal B-lymphocytes. In the USA, in adults, NHL is the 5th most common cancer, and of the NHL's themselves, diffuse large B-cell lymphoma is the most common type. About 10% originate from abnormal T-lymphocytes or NK (natural killer) cells of the immune system.
There are many types of non-Hodgkin lymphoma, so classifying which type it is can be difficult even for well-trained physicians. Careful study is performed on the cells' microscopic characteristics, since each is unique, as well as genetic studies that aid in differentiating them. They are also classified by how and where they grow in the human body, as well as their growth patterns and how they affect the patient. Each type is treated with specific treatment plans. Some are curable, some are not curable, most are treatable. The most up-to-date classification system is by the World Health Organization (WHO). According to the WHO, there are more than 80 subtypes, and more are being discovered and named all the time. Symptoms and signs range from slow and progressive to rapid and fatal. Sometimes it is curable or treatable, whereas other times it is ineffective.
B-lymphocytes are also called B-cells. When they are activated, they become plasma cells, which secrete antibodies in the form of immunoglobulins (Ig's). The plasma cells secrete 5 types of antibodies. They are immunoglobulin A (IgA), immunoglobulin G (IgG), immunoglobulin E (IgE), immunoglobulin M (IgM) and immunoglobulin D (IgD). T-lymphocytes are called "Helper Cells" because they "help" to activate B-cells to become activated to secrete specific antibodies to fight off disease.
There are two types of progressions:
- Slow-growing (indolent)
- Grow slowly
- A few symptoms, initially
- Generally incurable, but highly treatable
- Tend to respond well to treatment, so patients tend to live a long time with periods of remission (may be years or even decades)
- Some may transform into aggressive over time
- Types:
- Chronic lymphocytic leukemia/small lymphocytic lymphoma (CLL/SLL)
- Follicular lymphoma (FL)
- Lymphoplasmacytic lymphoma/Waldenström macroglobulinemia (WM)
- Marginal zone lymphoma (MZL)
- Mycosis fungoides (MF) (subtype of cutaneous T-cell lymphoma)
- Fast-growing (aggressive)
- Grow and spread quickly
- Often curable by treatments designed to kill rapidly-dividing tumor cells
- Types:
- Anaplastic large cell lymphoma (ALCL)
- Angioimmunoblastic T-cell lymphoma (AITL)
- Burkitt/Burkitt-like lymphomas
- Diffuse large B-cell lymphoma (DLBCL)
- Tends to have ups-and-downs
- May relapse (return)
- May become refractory (stop responding to treatment)
- Systemic
- R-CHOP therapy recommended
- Lymphoblastic leukemia/lymphoma Mantle cell lymphoma (MCL)
- Peripheral T-cell lymphoma, not otherwise specified (PTCL-NOS)
- Primary mediastinal large B-cell lymphoma (PMBL) (subtype of DLBCL)
- Aggressive
- Thought to rise from primary medullary B-cells
- 6-10% of all DLCBL's
- Associated with sclerosis
- Usually localized
- R-CHOP therapy recommended followed by mediastinal radiotherapy
- Better prognosis than other types
- Most can be cured
- 5-year survival rate: 75-85%
- Sézary syndrome (advanced subtype of cutaneous T-cell lymphoma)
- Painless enlargement of lymph nodes
- Fatigue
- Itching
- Bone pain
- Gastrointestinal disturbances
- Tonsils and adenoids may be enlarged
- Fever
- Night sweats
- Weight loss
Risk factors:
- Family history of any of the lymphomas
- Prior treatment with radiation, chemotherapy, immunotherapy
- Infection with HIV
- Infection with HTLV
- Infection with EBV (mononucleosis)
- Infection with hepatitis C
- Immunosuppression
- Connective tissue disorders like lupus or rheumatoid arthritis
- Crohn's disease, celiac disease or H. pylori infection (risk of GI lymphoma)
Treatment:
- Chemotherapy
Prognosis:
- Overall 5-year survival rate is about 53%
B-Cell Lymphomas:
A. Diffuse Large B-Cell Lymphoma
- Most common type (1 in 3 cases)
- Cells are large under the microscope
- Tends to affect older people (60's+)
- Quickly growing mass in a lymph node
- Fast-growing
- Responds well to treatment
- Cells appear large under the microscope
- Lots of fibrosis (scar tissue)
- About 2% of cases are this type
- Affects women more than men
- Affects women in their 30's
- Begins in the chest behind the breastbone (mediastinum)
- Presses on the windpipe leading to the lungs, and may cause trouble breathing
- If it blocks the Vena Cava, it can cause the arms and face to swell
- Fast-growing
- Responds well to treatment
- Rare
- Only found inside blood vessels
- 1 in 5 cases are this type
- Cells form a circular pattern around lymph nodes
- Tends to affect older people
- Affects lymph nodes around the body AND bone marrow
- Slow-growing
- Respond well to treatment, but difficult to cure
- 1 in 3 turn into the diffuse large B-cell lymphoma
- Closely related and different versions of the same disease
- Same type of cancer cell, but different area of the body
- CLL: blood and bone marrow; SLL: lymph nodes and spleen
- 5-10% of cases are this type
- Slow-growing but can convert to an aggressive type
- 5% of cases are this type
- Cell size: small to medium
- Widespread (lymph nodes, bone marrow and spleen)
- Not fast-growing, but difficult to treat
- 5-10% of cases are this type
- Small cells
- Three types:
- MALT Lymphomas (Extranodal Marginal Zone B-Cell Lymphoma or Mucosal-Associated Lymphoid Tissue)
- Begin outside the lymph nodes
- Most common
- Most begin in the stomach and are related to infection with Helicobacter pylori bacteria
- Many are linked to past bacterial or viral infections (oncoviruses)
- Average age of onset is 60+ years
- Slow-growing
- Often curable in early stages
- Nodal Marginal Zone B-Cell Lymphoma
- Rare
- Tends to affect older women
- Tends to stay localized in in the lymph node(s)
- Sometimes found in bone marrow
- Slow-growing
- Early stages easily cured
- Splenic Marginal Zone B-Cell Lymphoma
- Rare
- Occurs in spleen and bone marrow
- Tends to affect elderly
- Males more commonly affected
- Fatigue and enlarged spleen
- Linked to the Hepatitis C virus
- MALT Lymphomas (Extranodal Marginal Zone B-Cell Lymphoma or Mucosal-Associated Lymphoid Tissue)
- 1-2% of cases
- Medium cells
- Very fast-growing, aggressive cancer
- Tumor of jaw or facial bones in individuals of the African variety
- Linked to the Epstein-Barr Virus, which causes infectious mononucleosis or "mono" ("kissing disease") (African variety)
- Rare in the USA, and the type here is not usually linked to the virus
- Cases in the USA tend to begin as a mass in the abdomen, ovaries, testicles, or other organs, where it can spread to the brain and spinal cord
- 90% of the cases are male
- Average onset is 30
- Fast-growing, but about half of the cases are treated successfully
- Rare (only 1-2% of cases)
- Small cells
- Found in bone marrow, spleen and lymph nodes
- A type of lymphoma
- Rare (only about 700 cases/year)
- Small B-Lymphocytes with "hairy-like" projections of cytoplasm surrounding them
- Found in bone marrow, spleen and blood
- Tends to affect males more than females
- Tends to affect ages 50+
- Slow-growing
- Typically affects the brain
- May be found in spinal cord or tissues
- Tends to become widespread in the CNS
- Rare
- Tends to affect those with immunosuppression, such as those infected with HIV/AIDS
- Outlook is fairly poor
- Many types, but all are rare and make up <15% of all cases of Non-Hodgkin Lymphoma
- Accounts for <1% of cases
- Lymphomas have less bone marrow involvement than leukemias of the same type
- Small-to-medium, immature T-lymphocytes (lymphoblasts) are involved
- Usually starts in the thymus gland
- Can develop into a rather large mass or tumor in the chest (mediastinum)
- It can cause trouble breathing and can make the arms/face swell
- Most are young adults
- Males affected more than females
- Fast-growing
- Treatable if it hasn't spread to the bone marrow
- Rare
- Affect more mature T-cells
- Many Types:
- Cutaneous T-Cell Lymphomas (Mycosis Fungoides, Sezary Syndrome, Others)
- Begin in the skin
- About 5% of cases are this type
- Adult T-Cell Leukemia/Lymphoma
- Caused by infection with the virus HTLV-1
- Rare
- 4 types: Acute, Chronic, Smoldering, Lymphoma
- Angioimmunoblastic T-Cell Lymphoma
- About 3% of cases are of this type
- Tends to affect older adults
- Tends to affect lymph nodes, spleen or liver
- Fever, weight loss, rashes
- Tends to recur even when treated
- Extranodal Natural Killer/T-Cell Lymphoma Nasal Type
- Rare
- Affects the Upper Respiratory Tract
- May also affect the skin and digestive tract
- Enteropathy-Associated Intestinal T-Cell Lymphoma (EATL)
- Occurs in the intestinal lining and can cause obstructions, blockages, or perforations
- Type 1 (Gluten-sensitive enteropathy)
- Type 2 (Less common)
- Occurs in the intestinal lining and can cause obstructions, blockages, or perforations
- Anaplastic Large Cell Lymphoma
- 2% of cases
- Aggressive
- Tends to affect younger adults
- May start in the lymph nodes and spread to the skin
- Most cured with chemotherapy
- Primary Cutaneous Type (Skin)
- Systemic (Widespread)
- Peripheral T-Cell Lymphoma, Unspecified
- Any lymphomas that don't fit into the groups above
- Make up about 1/2 of all cases
- Tumor cells may be large or small
- Most are in their 60's
- Tend to be widespread and aggressive
- Long-term survival prognosis is not good
- Cutaneous T-Cell Lymphomas (Mycosis Fungoides, Sezary Syndrome, Others)
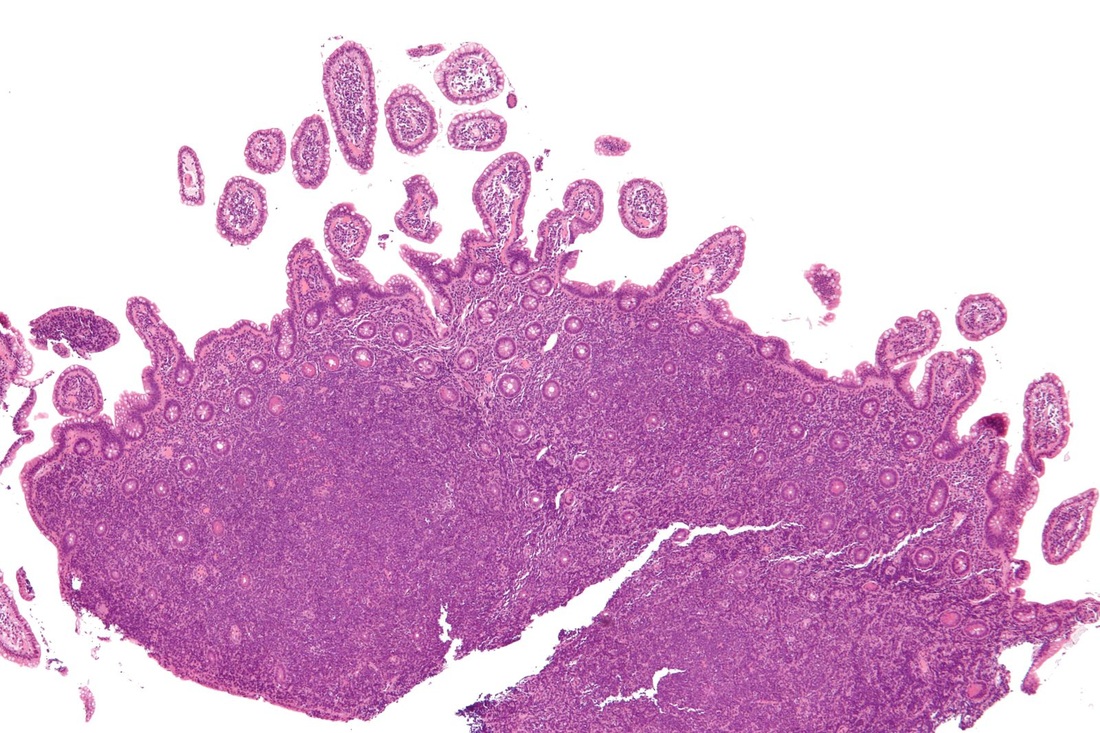
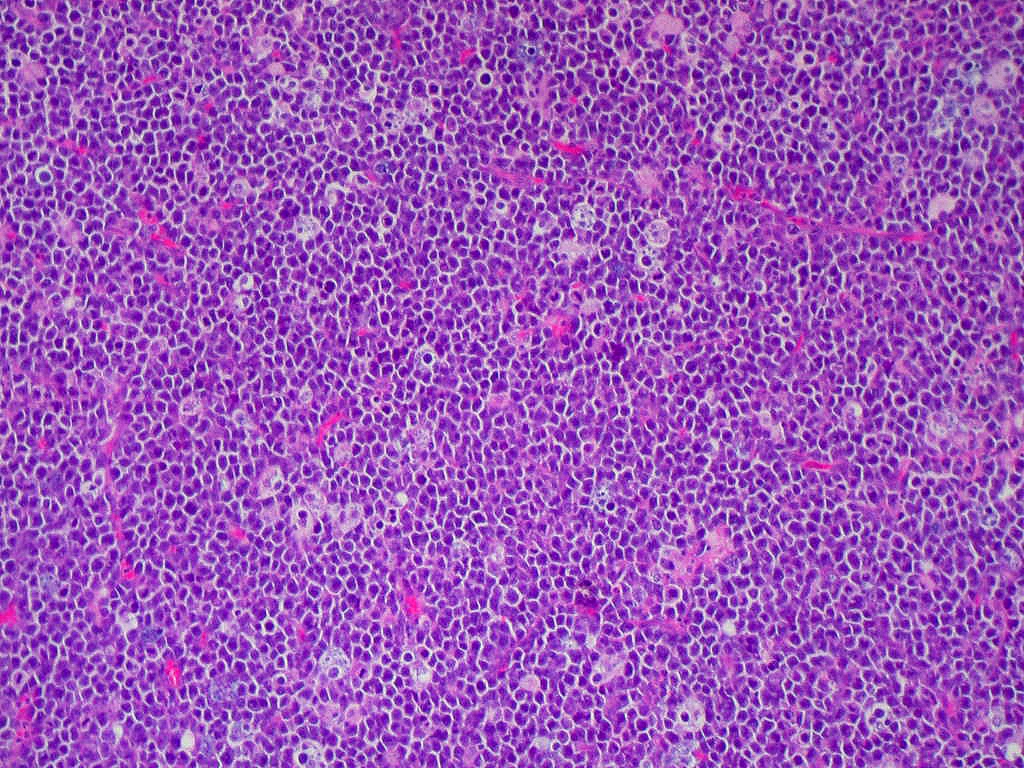
Lymphomas affect the lymphocytes of the immune system, and may affect B-lymphocytes or T-lymphocytes of different maturities. This one is affecting the B-lymphocytes. By Jensflorian - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=15184683
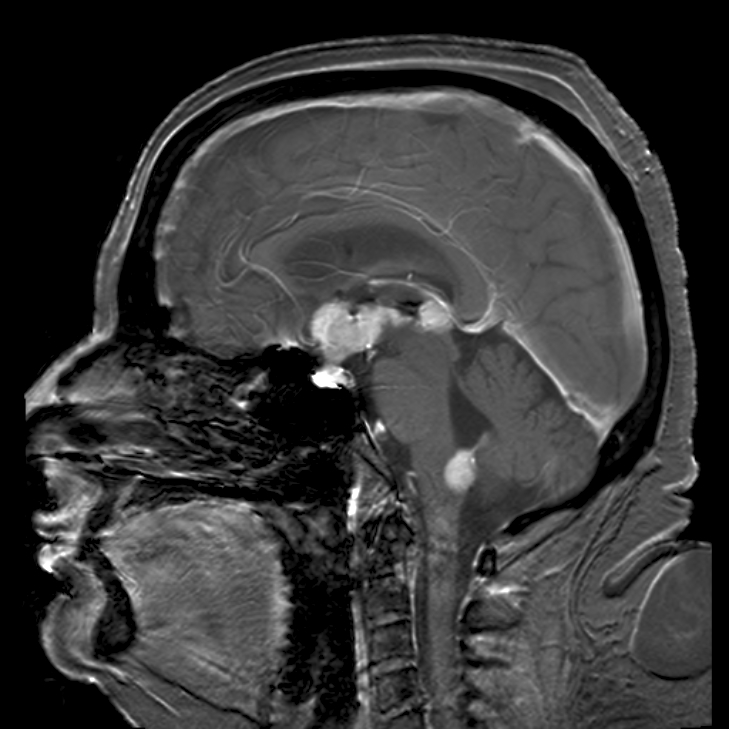
Lymphomas in the CNS; By Steven Fruitsmaak - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=6303862
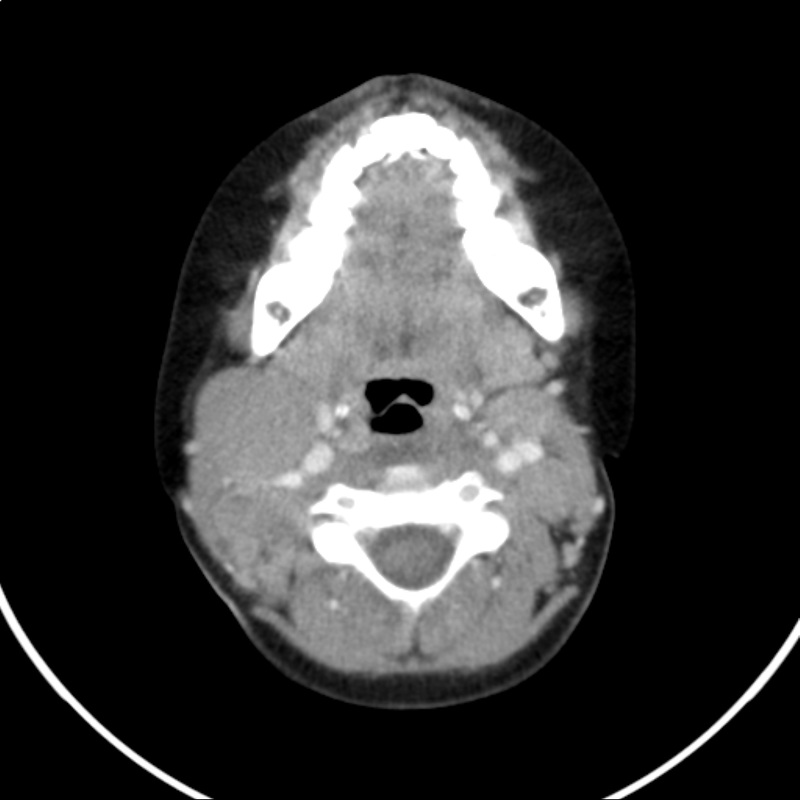
Lymphoma in the throat; By Christaras A - Created from anonymized dicom image., CC BY 2.5, https://commons.wikimedia.org/w/index.php?curid=1256258
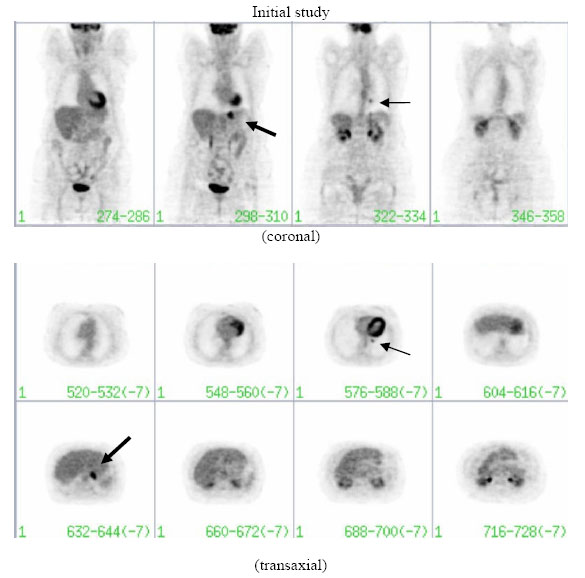
Lymphomas throughout the body; By Thomas EL, Lenzo NP, Troedson R - Gastric and pulmonary lymphoma presenting as a solitary pulmonary nodule, Biomed Imaging Interv J 2007; 3(4):e51. doi:10.2349/biij.3.4.e51., CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=4318299
Follicular Lymphoma; By Osaretin - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=51158891
Myelodysplastic Syndrome
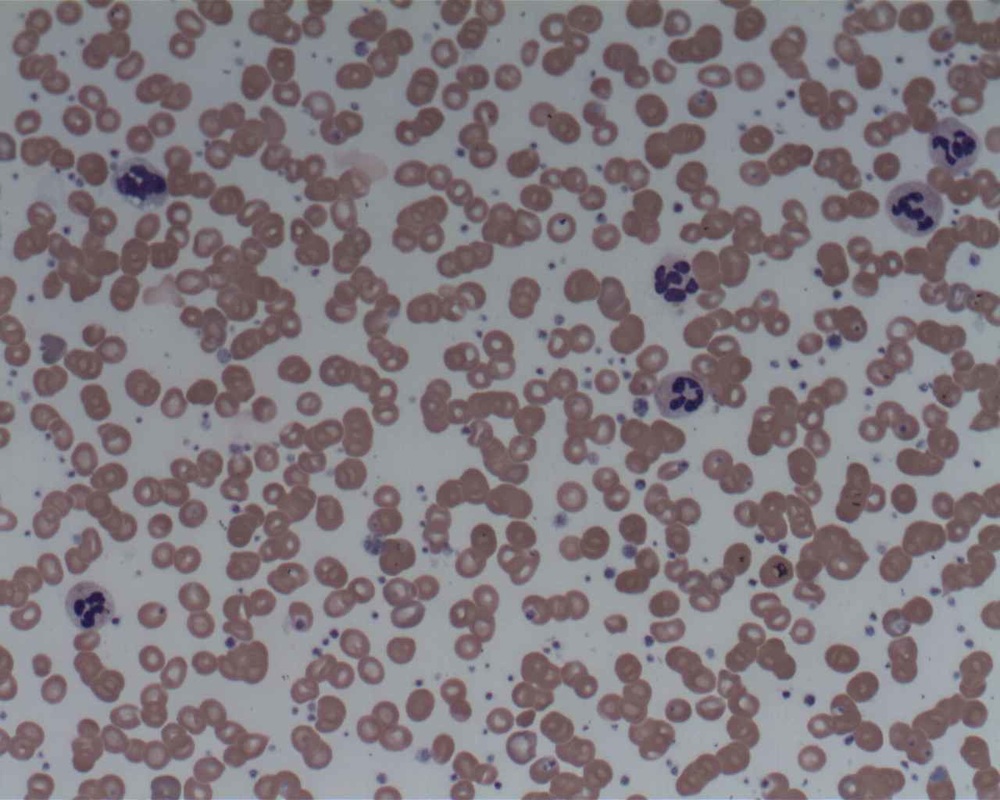
Myelodysplastic syndrome is a group of cancers that affects many cell types in the bone marrow. It affects immature cells, and they don't mature or become healthy. It also causes the red blood cells to stick together in stacks like coins (rouleaux). There are different types and they are classified based on which cells are affected and how they affect the blood and bone marrow. This type affects all cell types and maturities and causes changes in their shapes and behavior. There may be too many or too few cells.
Risks:
Symptoms:
Types:
A. Refractory Anemia
B. Refractory Anemia with Sideroblasts
D. Refractory Cytopenia with Multilineage Dysplasia
E. Refractory Cytopenia with Unilineage Dysplasia
F. Unclassifiable
G. Chromosome Abnormality del(q)
H. Chronic Myelomonocytic Leukemia (CMML)
Risks:
- Past radiation therapy or chemotherapy
- Exposure to radiation
- Age
- Tobacco smoke
- Pesticide exposure
- Fertilizer exposure
- Exposure to organic solvents like benzene
- Exposure to heavy metals like lead or mercury
Symptoms:
- Fatigue
- Shortness of breath
- Pale skin
- Easy bruising or bleeding
- Petechiae
Types:
A. Refractory Anemia
B. Refractory Anemia with Sideroblasts
- This type is associated with cells that have too much iron (they are sequestering iron)
D. Refractory Cytopenia with Multilineage Dysplasia
E. Refractory Cytopenia with Unilineage Dysplasia
F. Unclassifiable
G. Chromosome Abnormality del(q)
H. Chronic Myelomonocytic Leukemia (CMML)
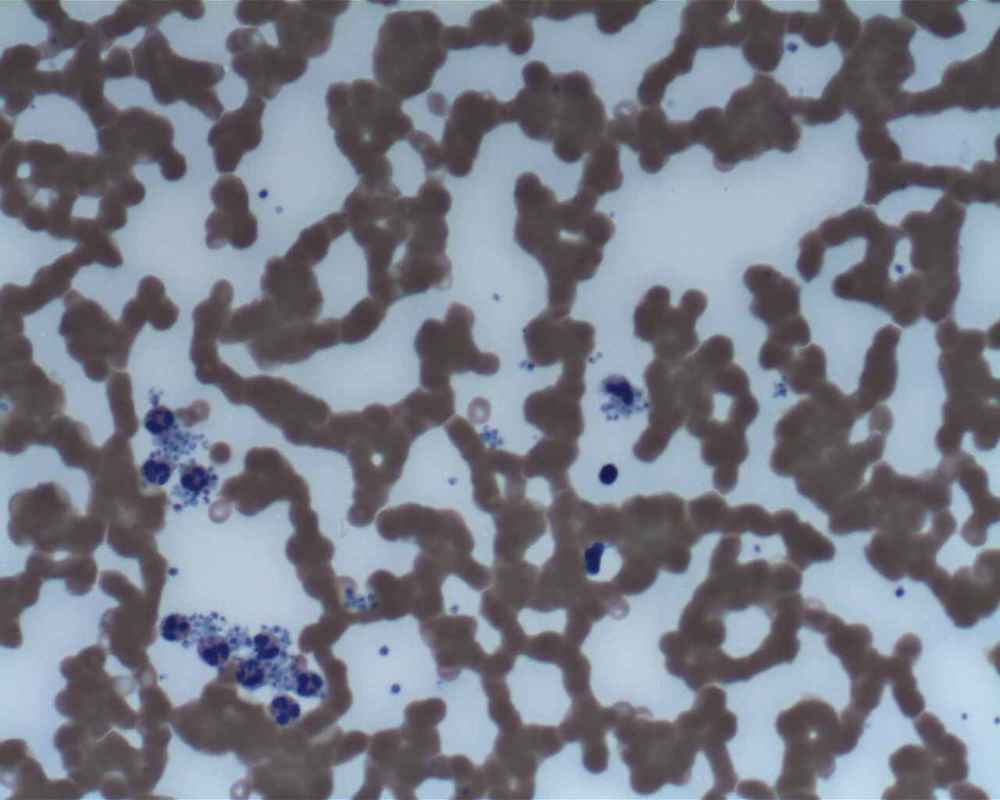
Myelodysplastic syndrome
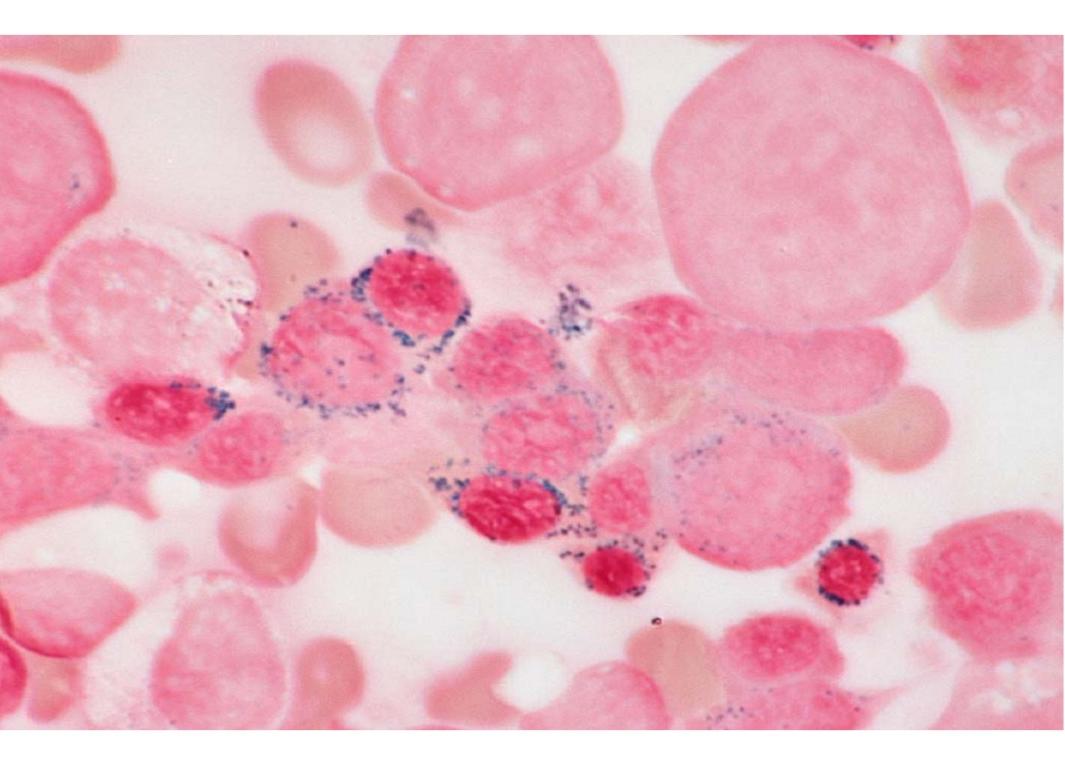
Myelodysplastic syndrome: This type is Refractory Anemia with Excess Sideroblasts. The blue represents excess iron. By TomskiiJA - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=17372254
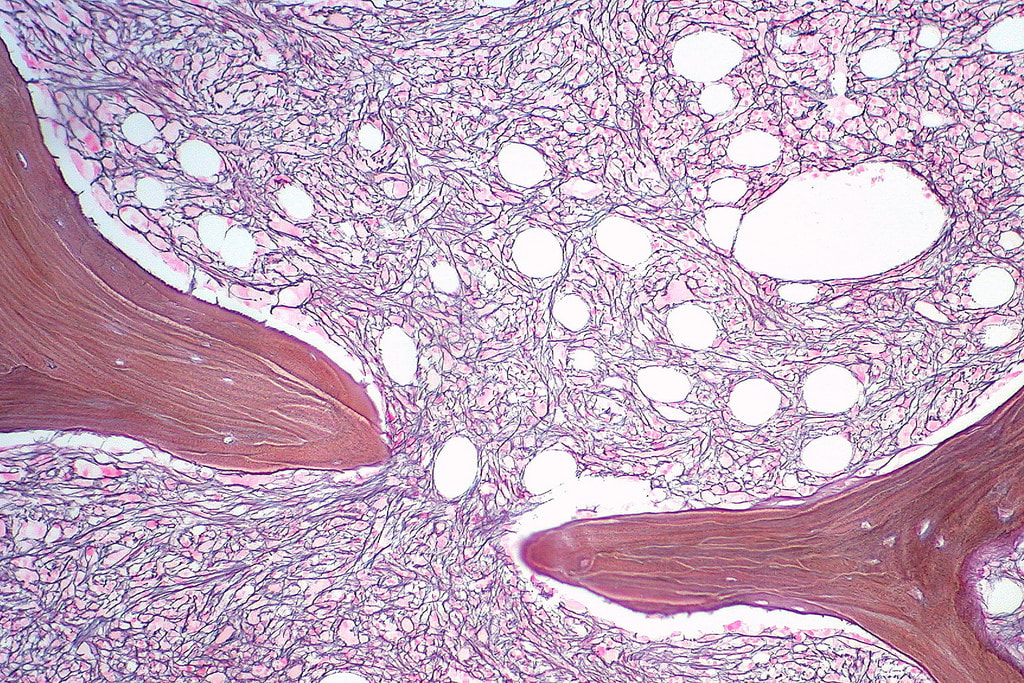
Myelofibrosis and dysplasia in the bone marrow; By TomskiiJA - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=17372251
Myelofibrosis with Mott cells seen
Myelodysplastic cells in the bone marrow affecting megakaryocytes; By The Armed Forces Institute of Pathology (AFIP) - PEIR Digital Library (Pathology image database). Image# 404740. Image and description are from the AFIP Atlas of Tumor Pathology.Declaration of PEIR: «Copyright Information - The Armed Forces Institute of Pathology Electronic Fascicles (CD-ROM Version of the Atlas of Tumor Pathology) contains both U.S. Government work and copyrighted materials used with permission of non-Government contributors. U.S. Government works may be used without restriction, but users of the Electronic Fascicle may not lawfully modify, rent, loan, distribute, create derivative works in whole or in part, or electronically transmit the copyrighted images from one computer to another or over a network without first obtaining permission from the copyright owners. All attempts have been made to remove copyrighted images from the PEIR Digital Library. If a copyright-protected image has inadvertently been included, please notify us and it will be removed immediately.», Public Domain, https://commons.wikimedia.org/w/index.php?curid=4345816
Myelofibrosis: Pelgroid cell, schistocytes, acanthocytes, bite cells, target cells); By The Armed Forces Institute of Pathology (AFIP) - PEIR Digital Library (Pathology image database). Image# 404814. Image and description are from the AFIP Atlas of Tumor Pathology.Declaration of PEIR: «Copyright Information - The Armed Forces Institute of Pathology Electronic Fascicles (CD-ROM Version of the Atlas of Tumor Pathology) contains both U.S. Government work and copyrighted materials used with permission of non-Government contributors. U.S. Government works may be used without restriction, but users of the Electronic Fascicle may not lawfully modify, rent, loan, distribute, create derivative works in whole or in part, or electronically transmit the copyrighted images from one computer to another or over a network without first obtaining permission from the copyright owners. All attempts have been made to remove copyrighted images from the PEIR Digital Library. If a copyright-protected image has inadvertently been included, please notify us and it will be removed immediately.», Public Domain, https://commons.wikimedia.org/w/index.php?curid=4345884
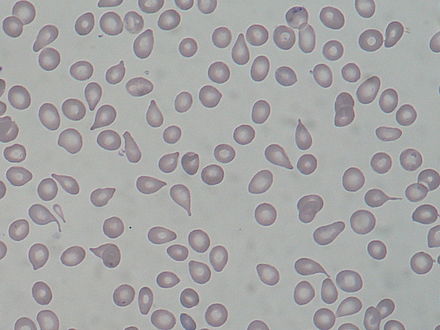
Dacrocytes/Poikilocytes (teardrop cells); By Osaretin - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=36814333
Giant platelets; By Bobjgalindo - Own work, GFDL, https://commons.wikimedia.org/w/index.php?curid=7761823
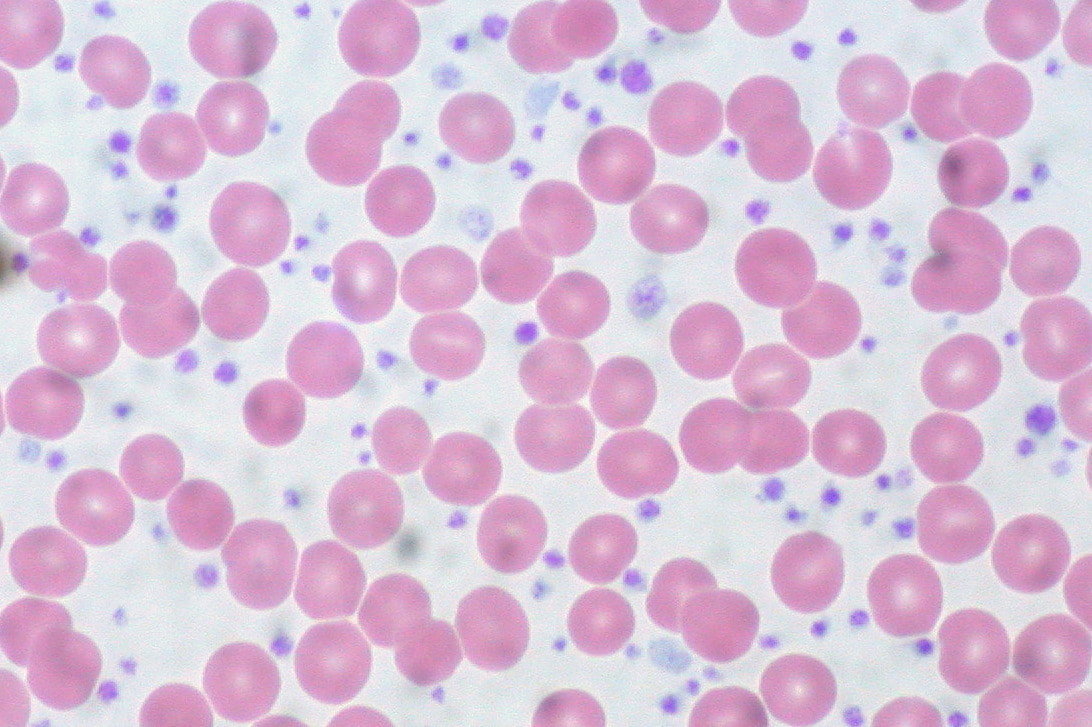
Thrombocytosis: Increase in the number of platelets; By Prof. Erhabor Osaro - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=36814530
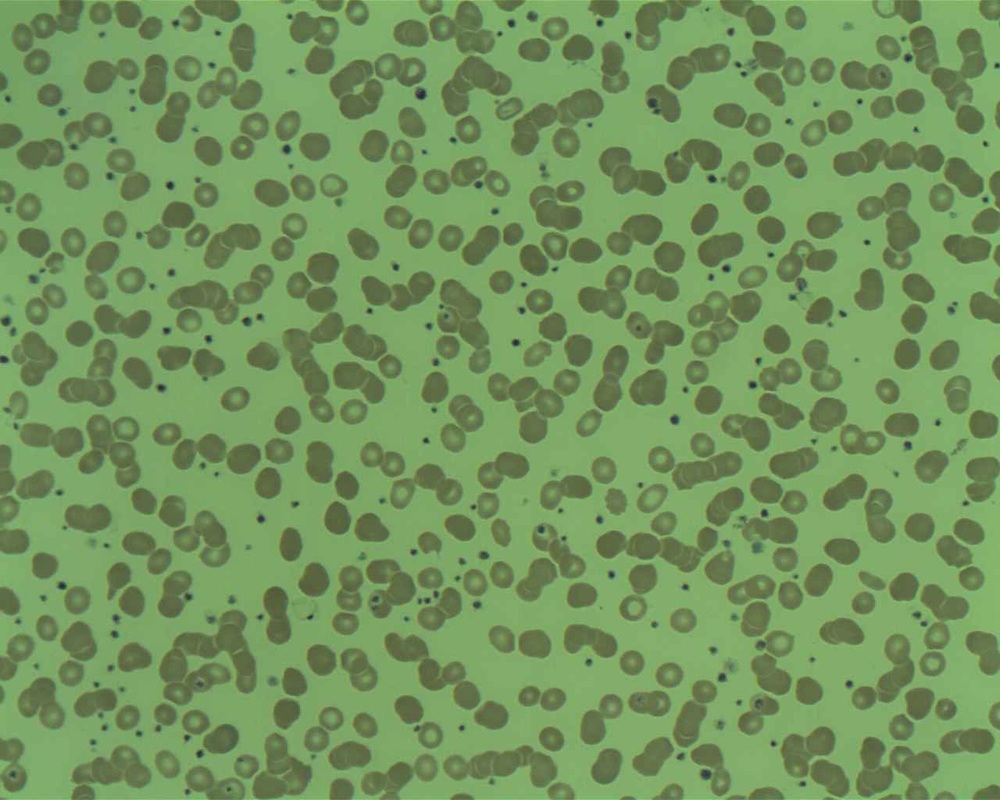
Thrombocytosis;By Prof. Erhabor Osaro - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=36814533
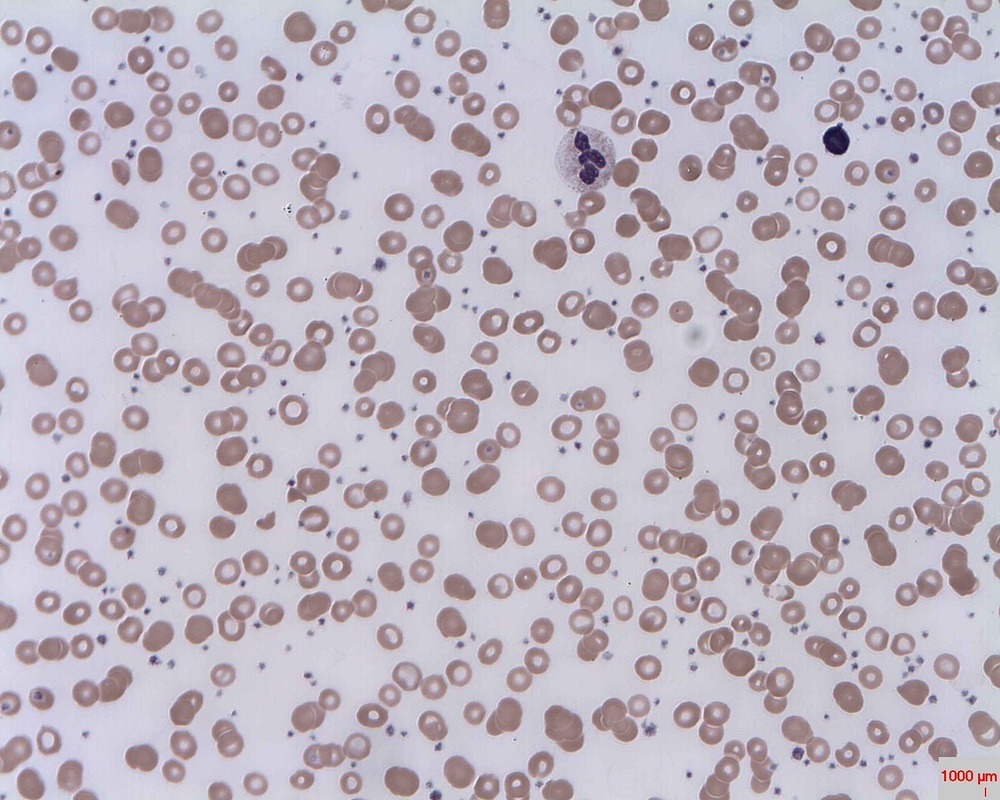
Thrombocytosis; By Erhabor Osaro (Associate Professor) - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=32131622
Myelofibrosis and poikilocytosis: variation in RBC size and morphology (schistocytes, elliptocytes, target cells, dacrocytes, microcytes, macrocytes, ovaloytes); By Osaretin - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=36814333
Myelofibrosis and poikilocytosis, a variation in red blood cell size and morphology (echinocytes, dacrocytes, ovalocytes, spherocytes, microcytes, macrocytes); By Prof. Osaro Erhabor - Prof. Osaro Erhabor, CC0, https://commons.wikimedia.org/w/index.php?curid=36793519
Mantle Cell Lymphoma Images:

By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=11219741

By Gabriel Caponetti - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=21994667
By Nephron - Own work, CC BY-SA 3.0, https://commons.wikimedia.org/w/index.php?curid=11219725
Platelet satellitism around neutrophils is seen in this type of lymphoma; By Osaretin - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=51158894
Burkitt's Lymphoma-African Variety:

This type causes tumors of the jaw and facial bones and is associated with the Epstein-Barr Virus; By Mike Blyth - Own work, CC BY-SA 2.5, https://commons.wikimedia.org/w/index.php?curid=1504829

By Mike Blyth - Own work, CC BY-SA 2.5, https://commons.wikimedia.org/w/index.php?curid=1504771
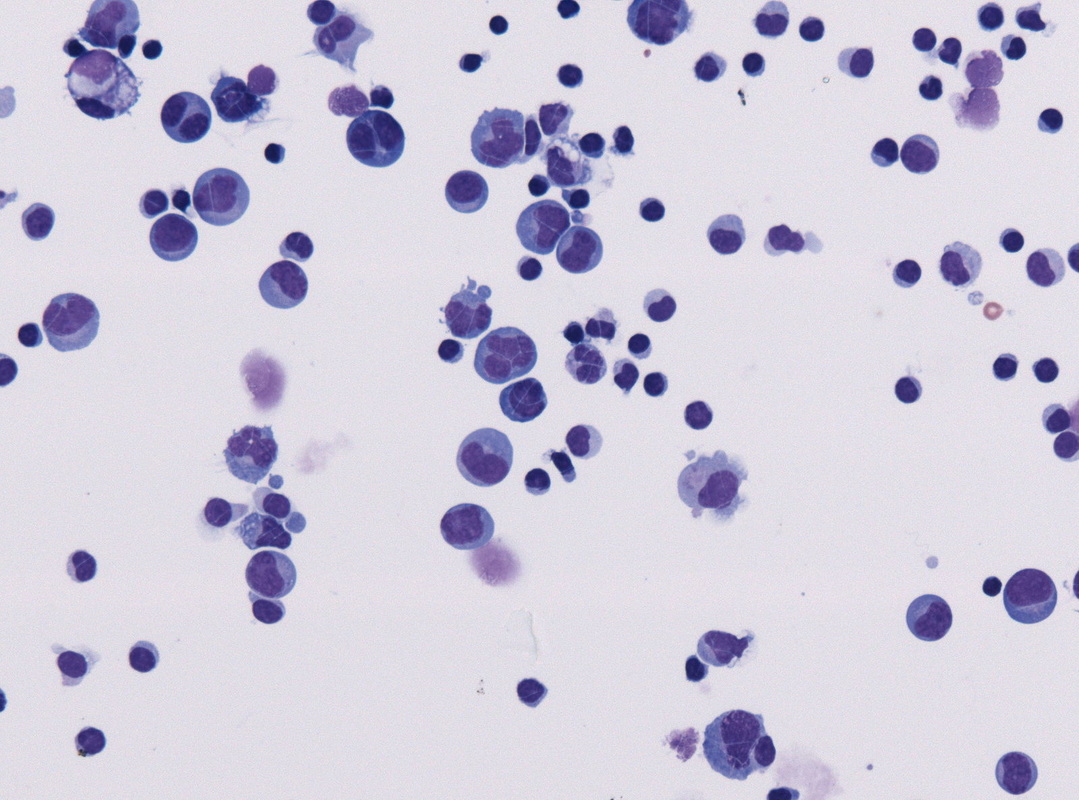
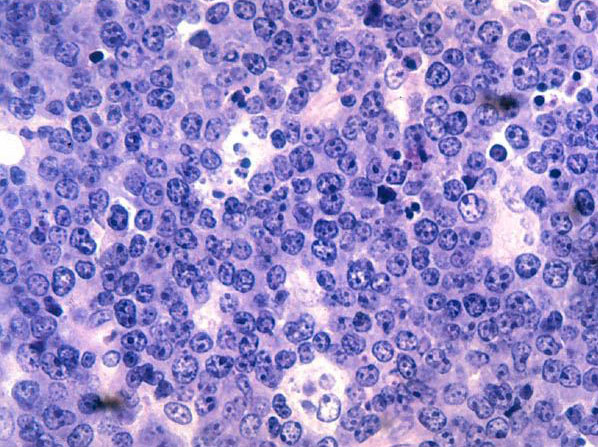
Burkitt's Lymphoma, Touch Prep, Wright's Stain.
This is a cancer of the B-lymphocytes, mainly occurring in the germinal center. There is an endemic form, a sporadic form and an immunodeficiency-form associated with the Epstein-Barr Virus (EBV). Prognosis is pretty good with early diagnosis and treatment, but can be poor if there are side-effects with the Chemotherapy. By Ed Uthman, MD. - http://flickr.com/photos/euthman/144136197/in/set-72057594114099781/, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1208814

By Ed Uthman from Houston, TX, USA - Burkitt Lymphoma (FNA, Giemsa stain)Uploaded by CFCF, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=30104277
By Ed Uthman from Houston, TX, USA - Burkitt Lymphoma (FNA, Giemsa stain)Uploaded by CFCF, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=30104278

By Ed Uthman from Houston, TX, USA - Burkitt Lymphoma (FNA, Pap stain)Uploaded by CFCF, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=30104274
By Ed Uthman from Houston, TX, USA - Burkitt Lymphoma (FNA, Pap stain)Uploaded by CFCF, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=30104275
By Ed Uthman from Houston, TX, USA - Burkitt lymphoma, H&EUploaded by CFCF, CC BY 2.0, https://commons.wikimedia.org/w/index.php?curid=30103521

By Ed Uthman, MD. - http://flickr.com/photos/euthman/144136195/in/set-72057594114099781/, Public Domain, https://commons.wikimedia.org/w/index.php?curid=1208807
By http://visualsonline.cancer.gov/details.cfm?imageid=4156, Public Domain, https://commons.wikimedia.org/w/index.php?curid=859300
http://commons.wikimedia.org/wiki/File:Epstein-barr_virus_%28ebv%29.jpg; http://www.cancer.gov;
https://visualsonline.cancer.gov/details.cfm?imageid=1948
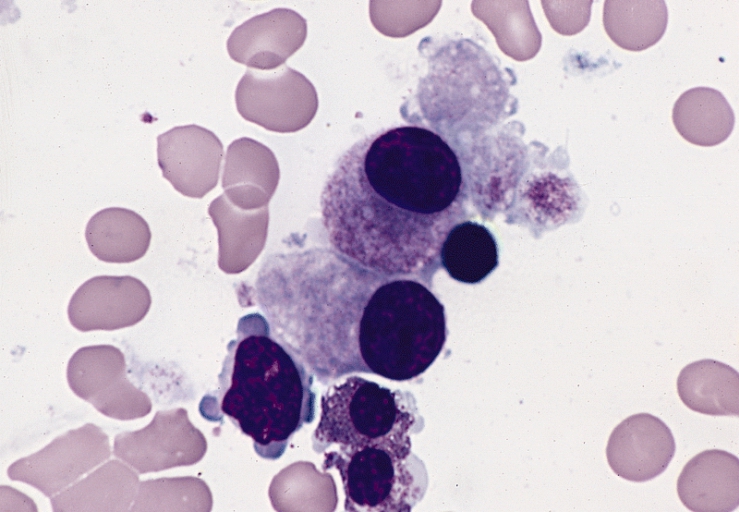
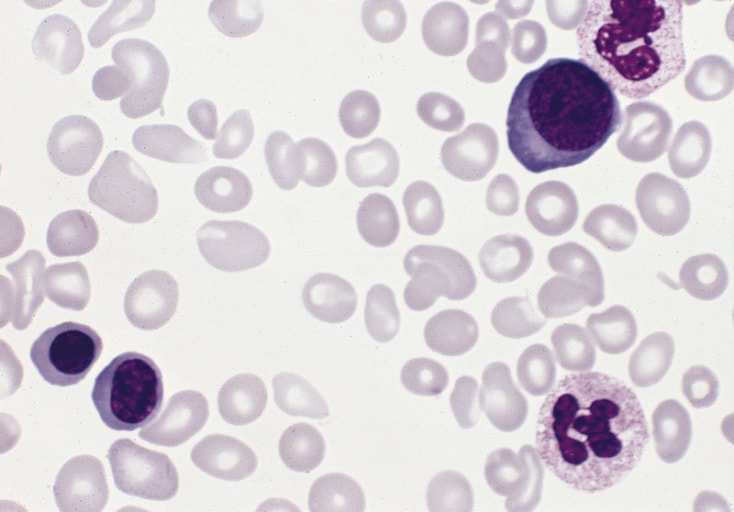
This image is of Infectious Mononucleosis reactive monocytes (monocytosis) caused by the Epstein-Barr Virus (EBV), which ca transform into malignant ones causing Burkitt's Lymphoma. Notice the heavy vacuolization and changes in shape from normal monocytes.
Mott Cell; By Osaretin - Own work, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=36814328
Acute Mast Cell Leukemia
Acute mast cell leukemia is a very rare variation of acute myeloid leukemia. It affects mast cells, or basophil granulocytes of the myeloid line. This type of leukemia may affect the internal organs, bone marrow, and/or even the skin (cutaneous lesions). When these cells proliferate, it causes intense systemic itching, due to the presence of the granules in the cytoplasm that release histamine, a substance that causing the symptoms of allergic reactions, such as itching, redness, watery eyes and nose, asthma, nausea, vomiting, chest and bone pain, fainting, dizziness, etc...
Sometimes this type can be familial (genetic). This type of leukemia is diagnosed by a variety of tests, including a blood chemistry test detecting blood serum tryptase.
Sometimes this type can be familial (genetic). This type of leukemia is diagnosed by a variety of tests, including a blood chemistry test detecting blood serum tryptase.

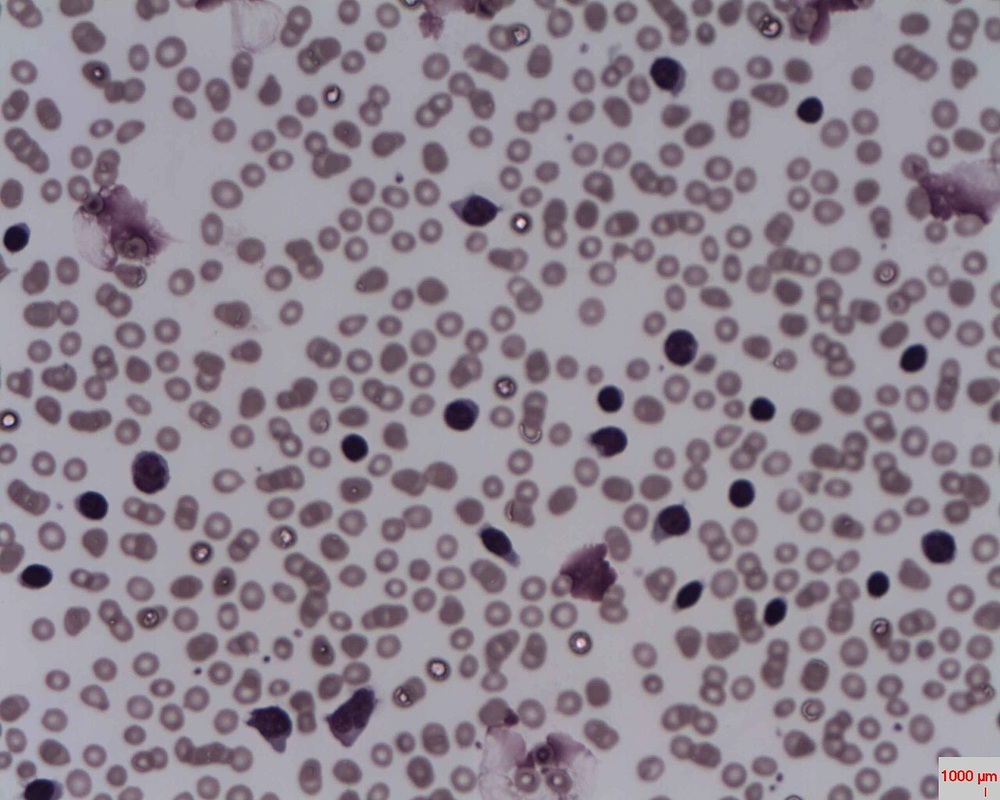
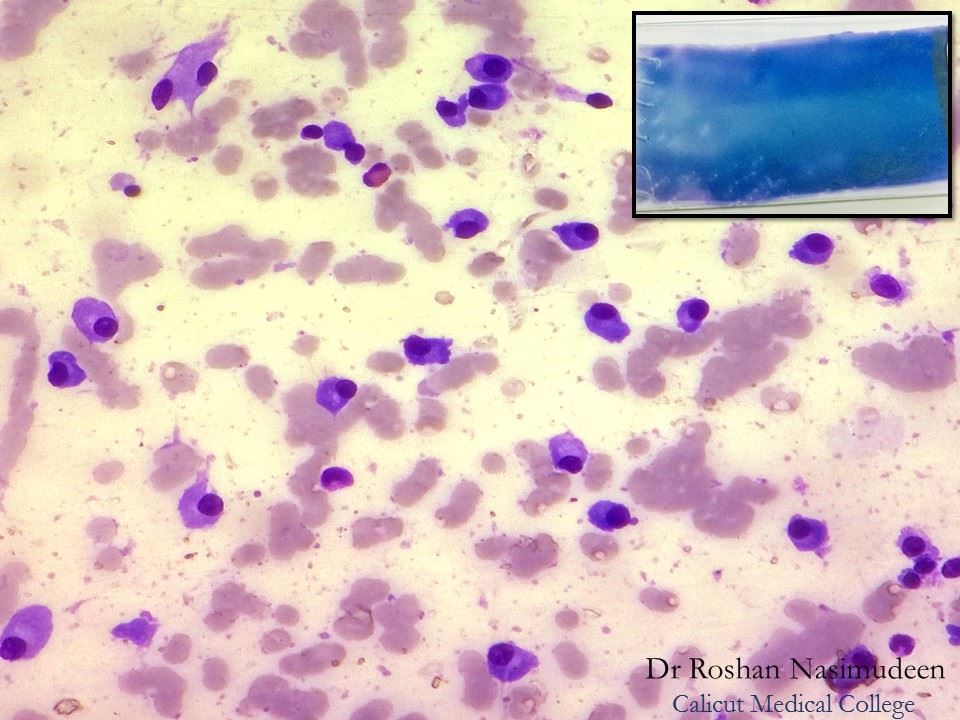
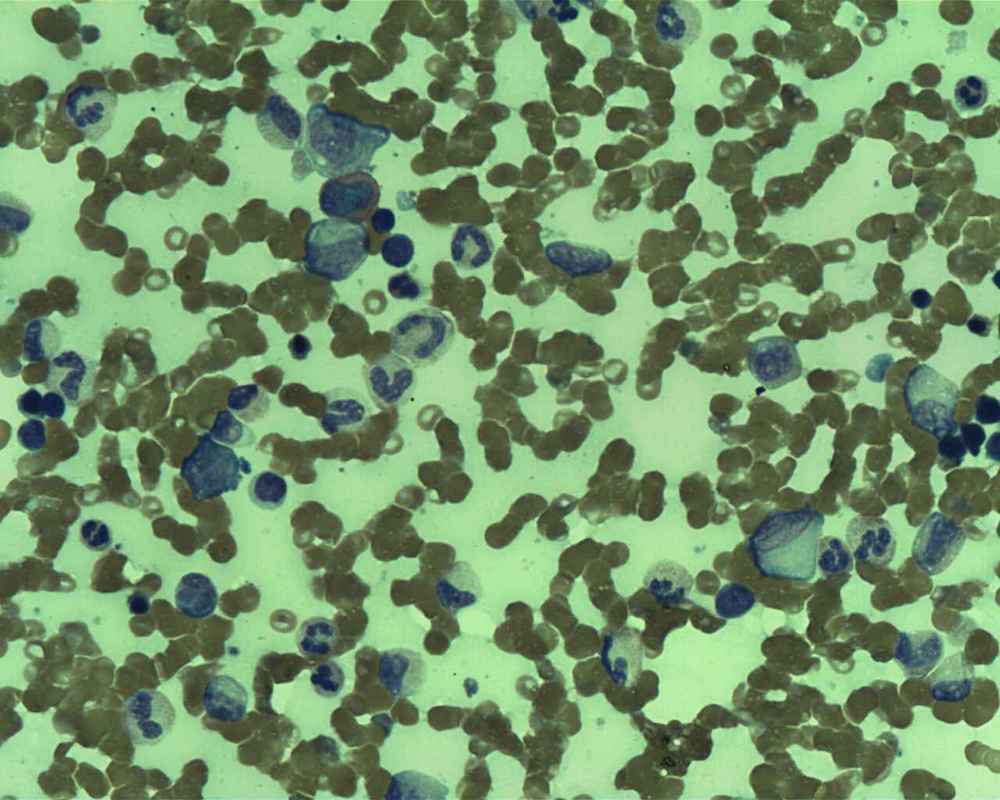
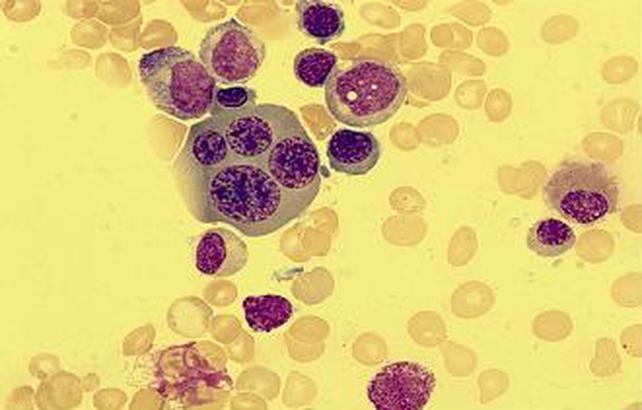
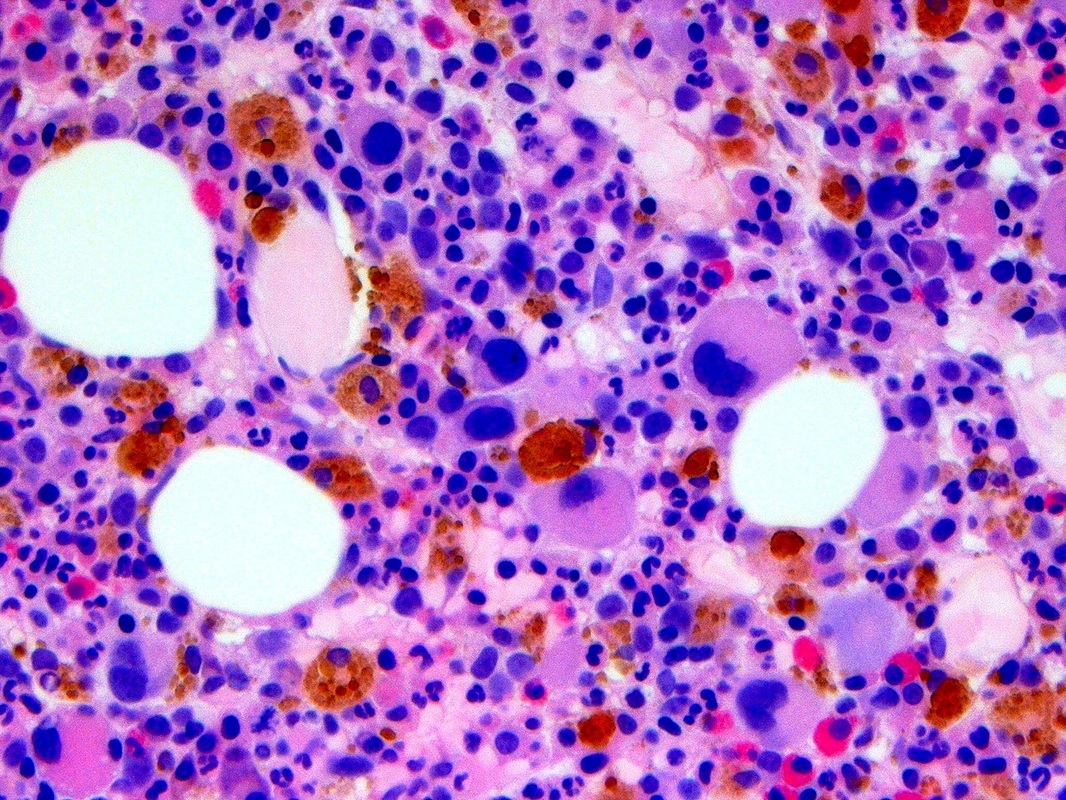
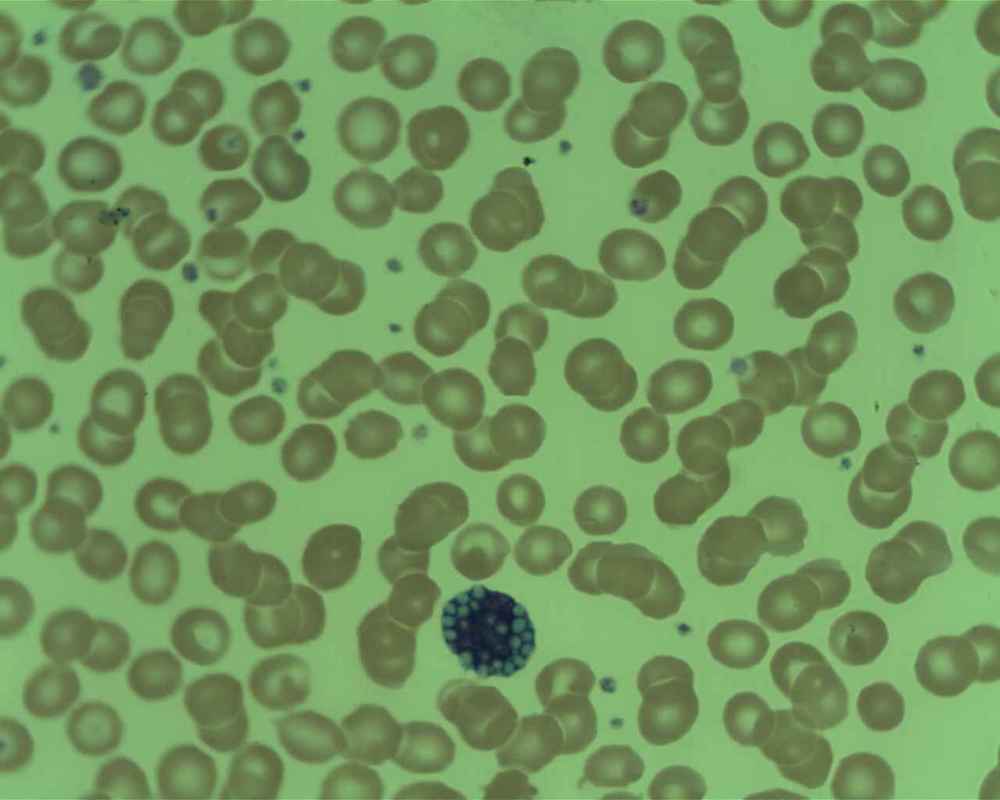
Mast Cell Leukemia is an aggressive type of AML. It can sometimes be a transformation from CML. WHO criteria for diagnosis includes at least 20% neoplastic mast cells seen in the bone marrow, and at least 10% neoplastic mast cells seen in the peripheral blood smear, as in the image here. The release of histamine by these cells results in symptoms such as headache, fever, flushing (trunk, face), stomach and bone pain, sometimes peptic ulcer, and hepatosplenomegaly. Release of heparin may result in bleeding and hemorrhage. This type has a poor prognosis, and survival from the time of diagnosis is usually only about 6 months. By Ayman Qasrawi at English Wikipedia - Transferred from en.wikipedia to Commons., Public Domain, https://commons.wikimedia.org/w/index.php?curid=35421736
Polycythemia Vera (PV):
Essential Thrombocythemia:
Thrombocythemia is another term for thrombocytosis, or an increase in the amount of platelets.
Myelofibrosis With Myloid Metaplasia (MMM):
References:
- The American Cancer Society: https://www.cancer.org/cancer/non-hodgkin-lymphoma/about/types-of-non-hodgkin-lymphoma.html
- Mayo Clinic: https://www.mayoclinic.org
- National Cancer Institute: https://www.cancer.gov
- Leukemia and Lymphoma Society: https://www.lls.org
- Lymphoma Research Foundation: https://www.lymphoma.org
- National Library of Medicine: https://pubmed.ncbi.nlm.nih.gov/31414888/
- Lymphoma.org: https://lymphoma.org/wp-content/uploads/2021/04/LRF-NHL-Booklet_4.21.pdf
