Collecting and Processing Blood Specimens:
Quality Assurance and Quality Control:
Quality patient care, excellence and accuracy begins with the quality of the specimen that is collected and properly labeled and sent to the laboratory. Phlebotomists, laboratory scientists and technicians, and nurses play a key role in quality patient care, starting with pre-analytical preparation.
The sample quality depends upon a number of factors:
Sample quality determines if the sample will be able to be tested and determines the quality of the testing ability itself. Improper collection, storage, transportation, mislabeling or handling in any manner will render testing invalid, if not impossible, which may delay diagnosis and treatment, cause inconvenience or pain to the patient, and require a redraw/recollection. There is a lot of factors to keep in mind when collecting patient samples. It is helpful to think of the patients you work with as your own family and friends or yourself and how you would want to be treated.
The pre-analytical steps are referred to as quality assurance or quality assessment, and quality control. This involves everyone on the healthcare team. It is used to describe management of the treatment of the entire patient as an individual, and includes everything from making sure that ranges are set, collection devices are in date and not expired, to testing reagents ahead of time, making sure labels are correct and the patient is correctly identified and samples are correctly labeled, to making sure that all paperwork is complete and correct, and many things in between.
This begins with the establishment of policies and procedures that are followed for consistency, including standard operating procedures that are maintained, updated and controlled and guide laboratory collection and assessment of specimens. These include a number of measures, including:
The sample quality depends upon a number of factors:
- How the sample was collected
- How the sample was transported
- How the sample was processed or preserved
Sample quality determines if the sample will be able to be tested and determines the quality of the testing ability itself. Improper collection, storage, transportation, mislabeling or handling in any manner will render testing invalid, if not impossible, which may delay diagnosis and treatment, cause inconvenience or pain to the patient, and require a redraw/recollection. There is a lot of factors to keep in mind when collecting patient samples. It is helpful to think of the patients you work with as your own family and friends or yourself and how you would want to be treated.
The pre-analytical steps are referred to as quality assurance or quality assessment, and quality control. This involves everyone on the healthcare team. It is used to describe management of the treatment of the entire patient as an individual, and includes everything from making sure that ranges are set, collection devices are in date and not expired, to testing reagents ahead of time, making sure labels are correct and the patient is correctly identified and samples are correctly labeled, to making sure that all paperwork is complete and correct, and many things in between.
This begins with the establishment of policies and procedures that are followed for consistency, including standard operating procedures that are maintained, updated and controlled and guide laboratory collection and assessment of specimens. These include a number of measures, including:
- Preparing the patient prior to any specimens being collected
- Collecting valid samples by following procedures for collection
- Transporting the sample correctly, whether it be protected from light, on ice, upright, at room temperature, frozen, padded, wrapped in parafilm, or whatever specific steps are required for that particular sample
- Making sure there is a test order or requisition and that it is followed for analysis, including any add-ons or modifications by the provider
- Validation of test results
- Recording and reporting the assay results within the proper turnaround time and reporting STAT test results immediately
- Releasing results in the LIS by transmitting them to the patient's chart
- Documenting everything, including any problems, QC performance, equipment maintenance, adverse events or reactions, availability of records, proper dates and times of collection, initials, records describing quality assurance practices and quality control methods (daily, weekly, monthly, biannually, annually, quarterly, etc...)
- Making sure that you keep up with your certifications, CEU's, training, proficiency surveys, whatever is required by your facility
The Role of the Phlebotomist and Patient Care:
The role of the phlebotomist and other healthcare providers who collect blood is crucial and begins the process of collection, testing, analysis, results/diagnosis and treatment. It is so important to the laboratory and to the patient and their satisfaction and quality of care.
Believe it or not, more than 2/3rd's of laboratory errors are caused by errors and mistakes that occur prior to testing, during the pre-analytical phase, many being related to sample collection and handling. This includes everything from collecting the wrong tube, mislabeling, forgetting to label a sample, failing to document the date and time of collection, a lost tube (rolls under a cart, falls into the trash can, rolls under a courier's seat, etc...), a hemolyzed sample, failing to remove the tourniquet within a minute, labeling the wrong tube (getting patients mixed up), failure to properly identify the patient, drawing from an IV line, failure to flush the tube first (discard tubes), or others.
By being vigilant and aware, the phlebotomist has the important role in being a person who can reduce these mistakes by being well-trained, confident, having integrity, and always being alert to things that can be sources of error. The phlebotomist is also able to be a source of comfort and education to the patient, reassuring them and explaining to them the reason for the sample collection and what it will be used for.
It is important to be relaxed yourself, kind, gentle, compassionate, friendly, helpful, show respect and genuine concern for the patient and their interests, make good eye contact, be a good listener, address any questions or concerns or complaints the patient has, be tactful and diplomatic, patient, and do what you can to resolve any issues by offering to find a solution and by apologizing on behalf of the healthcare team and by rectifying it.
You should strive to address the patient by their formal title (Dr., Mr., Mrs., Miss, Ms.) rather than simply by their first name. If you notice that they have difficulty hearing or processing the information, speak slightly slower and louder, enunciating your words clearly, followed by asking them if they have any questions and if they understand.
It is also important to take your time and not rush and allow enough time for the procedure in order to avoid mistakes. Double-check all information. Take extra time, if needed, to gain the confidence and trust of the patient, especially pediatric patients. Complete integrity and honesty is of utmost importance, and patients should be initially greeted in a friendly, warm manner, creating a calm, pleasant environment.
The healthcare system is a team of people, and all individuals and departments equally matter and are of equal importance in the entire patient experience. The patient's rights should be considered at all times and their privacy should be respected. It should be the goal of all healthcare providers to provide:
Believe it or not, more than 2/3rd's of laboratory errors are caused by errors and mistakes that occur prior to testing, during the pre-analytical phase, many being related to sample collection and handling. This includes everything from collecting the wrong tube, mislabeling, forgetting to label a sample, failing to document the date and time of collection, a lost tube (rolls under a cart, falls into the trash can, rolls under a courier's seat, etc...), a hemolyzed sample, failing to remove the tourniquet within a minute, labeling the wrong tube (getting patients mixed up), failure to properly identify the patient, drawing from an IV line, failure to flush the tube first (discard tubes), or others.
By being vigilant and aware, the phlebotomist has the important role in being a person who can reduce these mistakes by being well-trained, confident, having integrity, and always being alert to things that can be sources of error. The phlebotomist is also able to be a source of comfort and education to the patient, reassuring them and explaining to them the reason for the sample collection and what it will be used for.
It is important to be relaxed yourself, kind, gentle, compassionate, friendly, helpful, show respect and genuine concern for the patient and their interests, make good eye contact, be a good listener, address any questions or concerns or complaints the patient has, be tactful and diplomatic, patient, and do what you can to resolve any issues by offering to find a solution and by apologizing on behalf of the healthcare team and by rectifying it.
You should strive to address the patient by their formal title (Dr., Mr., Mrs., Miss, Ms.) rather than simply by their first name. If you notice that they have difficulty hearing or processing the information, speak slightly slower and louder, enunciating your words clearly, followed by asking them if they have any questions and if they understand.
It is also important to take your time and not rush and allow enough time for the procedure in order to avoid mistakes. Double-check all information. Take extra time, if needed, to gain the confidence and trust of the patient, especially pediatric patients. Complete integrity and honesty is of utmost importance, and patients should be initially greeted in a friendly, warm manner, creating a calm, pleasant environment.
The healthcare system is a team of people, and all individuals and departments equally matter and are of equal importance in the entire patient experience. The patient's rights should be considered at all times and their privacy should be respected. It should be the goal of all healthcare providers to provide:
- high-quality, excellent care
- provide a safe and clean environment
- involvement of the patient in their care decisions
- protection for their privacy by maintaining confidentiality
- help and aid for patients entering and leaving the hospital, whether it be offering them help to and from their vehicle or ride, a wheelchair or your arm, help finding where to go, helping them carry their belongings if you see that their hands are full, help if they do not speak English by offering to help them find an interpreter
- guidance for where to go and who to talk to regarding admissions, records, registration, billing and insurance
- information about how a patient can choose a proxy or decision maker that can make decisions on their behalf if they are unable to
- any forms needed to be filled out or signed, pamphlets, and providing oral explanation of the steps involved, test procedures, preparation, and by answering any questions they may have
Infection Control, Isolation and Precautions:
Some important key concepts and medical terminology fall under infection control, isolation and precaution measures. They are as follows:
- Isolation: a set of special precautions and a safety system that is routinely practiced by healthcare personnel to ensure the safest environment possible throughout the healthcare facility
- Standard Precautions:
- First tier of infection control
- Goal is to reduce the risk of microbial transmission and infection, including that of HIV, from both identified and unidentified sources of infection
- Series of protocols followed whenever contact is made with blood or body fluids
- Includes universal precautions, which means to treat all blood and body fluids as if they are infected with HIV
- First tier of infection control
- Special Precautions:
- Second tier of infection control
- Provide additional precautions to control transmission of infectious agents of disease when standard precautions are not enough
- Contact Precautions
- Stop the spread of microbes via direct contact
- Skin-to-skin
- Skin-to-skin
- Stop the spread of microbes via indirect contact
- Contaminated, inanimate object (fomite), such as a surface, doorknob, clothing or linens
- Contaminated, inanimate object (fomite), such as a surface, doorknob, clothing or linens
- Includes wearing PPE (personal protective equipment):
- Gloves
- Gowns (if on isolation)
- Masks
- Gloves
- Stop the spread of microbes via direct contact
- Airborne Precautions
- Designed to prevent extremely tiny airborne bacterial or viral particles or dust particles from transmitting disease, since they may be suspended in the air for an extended period of time
- Respiratory protection is required (N95 or CPAP)
- Designed to prevent extremely tiny airborne bacterial or viral particles or dust particles from transmitting disease, since they may be suspended in the air for an extended period of time
- Droplet Precautions
- Protect the healthcare worker AND the patient and other visitors from droplets, which may be expelled during coughing, sneezing, breathing, singing, talking
- Mask is required, and a gown may be required as well
- Negative pressure air room is required
- Protect the healthcare worker AND the patient and other visitors from droplets, which may be expelled during coughing, sneezing, breathing, singing, talking
- Second tier of infection control
Specimen Collection:
Blood is the most frequent type of specimen collected and analyzed in the clinical laboratory, though many different types of samples are collected and analyzed. This website focuses on collection and analysis of blood.
I focus on collection and analysis of urine and body fluids at https://www.urinalysisandbodyfluids.weebly.com. You can find out more about microbiology analysis at https://www.microbiologylearning.weebly.com. For specific information about serum and plasma chemistry and immunology testing, see https://www.jensbasicchemistry.weebly.com. For pathophysiology and diseases affecting human body systems, see https://www.essentialsofanatomyandphysiology.weebly.com.
I focus on collection and analysis of urine and body fluids at https://www.urinalysisandbodyfluids.weebly.com. You can find out more about microbiology analysis at https://www.microbiologylearning.weebly.com. For specific information about serum and plasma chemistry and immunology testing, see https://www.jensbasicchemistry.weebly.com. For pathophysiology and diseases affecting human body systems, see https://www.essentialsofanatomyandphysiology.weebly.com.
Blood Collection Factors:
Laboratory collection, testing and analysis on blood tends to take place on whole blood, plasma or serum. These specimens may be drawn from a fasting or nonfasting state, but it is important to know which tests you are drawing for require fasting and which ones do not, so you can ask your patient if they have fasted or not.
A fasting state is defined as having no food or liquid other than water for about 8-12 hours prior to blood collection. For most lab tests, this is not necessary, however, for things like blood glucose and testing for diabetes or for managing diabetes, fasting is required. These samples should be collected ASAP in the morning before breakfast. Food, beverages, activity and exercise, time of day and medications are all factors or variables that can influence laboratory test results.
If blood is collected right after a meal, it is referred to as postprandial. There are cases where blood glucose levels are checked 2 hours postprandial, or 2 hours after a meal. After this time, in patients without diabetes, the blood sugar levels typically return to normal or to almost fasting levels, however, in diabetic patients, this may not be the case, aiding in diagnosis or monitoring their condition, treatment or therapy.
When a patient is receiving IV therapy, blood should not be drawn during this time. Either wait, or turn off the IV for 10-20 minutes, then collect the blood from the opposite arm, only after filling 2 flush tubes (discard tubes) that you throw away before collecting blood to be sent to the lab for analysis.
Other variables include the following:
A fasting state is defined as having no food or liquid other than water for about 8-12 hours prior to blood collection. For most lab tests, this is not necessary, however, for things like blood glucose and testing for diabetes or for managing diabetes, fasting is required. These samples should be collected ASAP in the morning before breakfast. Food, beverages, activity and exercise, time of day and medications are all factors or variables that can influence laboratory test results.
If blood is collected right after a meal, it is referred to as postprandial. There are cases where blood glucose levels are checked 2 hours postprandial, or 2 hours after a meal. After this time, in patients without diabetes, the blood sugar levels typically return to normal or to almost fasting levels, however, in diabetic patients, this may not be the case, aiding in diagnosis or monitoring their condition, treatment or therapy.
When a patient is receiving IV therapy, blood should not be drawn during this time. Either wait, or turn off the IV for 10-20 minutes, then collect the blood from the opposite arm, only after filling 2 flush tubes (discard tubes) that you throw away before collecting blood to be sent to the lab for analysis.
Other variables include the following:
- Patient position (sitting up, lying down or standing)
- Immobilization (prolonged bed rest)
- Exercise
- Recent food or caffeine ingestion
- Circadian rhythm
- Smoking
- Alcohol use
- Administration of drugs (example: blood thinners, aspirin, insulin, etc...)
- Underlying conditions
Procedures:
In general, two major sources of blood are used for clinical lab testing:
- Peripheral blood (capillary)
- Collected by skin puncture
- Finger stick
- Use the fingertip of the 3rd or 4th finger
- Use the fingertip of the 3rd or 4th finger
- Heel stick
- Do not use the middle of the foot or toes, rather use the outer third or inner third (medial or lateral) of the foot
- Do not use the middle of the foot or toes, rather use the outer third or inner third (medial or lateral) of the foot
- Ear lobe
- This is should be used ONLY as a last resort and ONLY in adult patients
- This is should be used ONLY as a last resort and ONLY in adult patients
- Finger stick
- Useful for point-of-care testing
- Common test: bedside testing for glucose using a handheld device and commercial reagent sticks
- 1-2 minute test
- 1-2 minute test
- Other: testing of infants for phenylketonuria, hereditary galactosemia, hypothyroidism, hemoglobinopathies like sickle cell or thalassemia
- Blood should be collected 1-3 days after birth and before the infant is discharged from the hospital and at least 24 hours after birth
- Usually performed by heel stick and collected on a filter paper card that is sent to the lab for analysis
- The drop of blood is touched to a circle imprinted on the filter paper card until the circle is completely filled, and allowed to fully air-dry
- Blood should be collected 1-3 days after birth and before the infant is discharged from the hospital and at least 24 hours after birth
- Collected by skin puncture
- Venous blood (veins)
- Collected by phlebotomy, or venipuncture
- See information below and on the next tab: Phlebotomy and Venipuncture
- See information below and on the next tab: Phlebotomy and Venipuncture
- Collected by phlebotomy, or venipuncture

Venipuncture Procedure and Supplies:
Blood collection has grown safer through the years thanks to development of products and an increase focus on safety. These are designed to product both the blood collector and the patient. Some of the most commonly used products are:
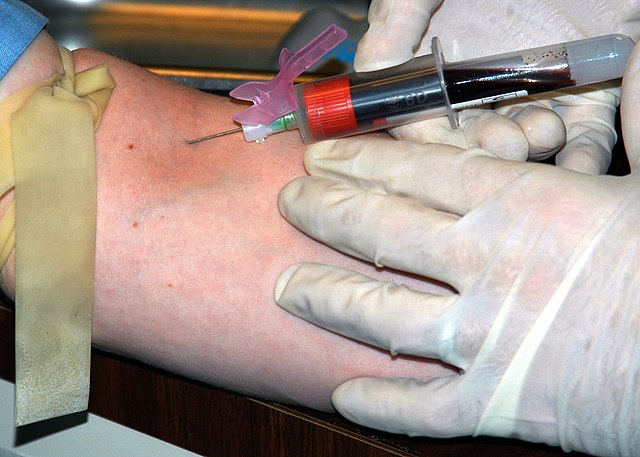
The standard needle used for blood collection procedures is the 21-gauge needle with either a syringe or the evacuated blood collection tubes. The needle is double-ended. The longer end is the one used to collect blood from the patient's vein, and the shorter end is used to pierce the rubber stopper of the evacuated tube.
In general, the higher the gauge number, the smaller the bore (inner diameter) of the needle. The single-use, plastic needle holder is used to secure the needle to the syringe, and the plastic safety feature is a plastic needle cover to be used immediately after blood collection with one hand to prevent an accidental needle stick.
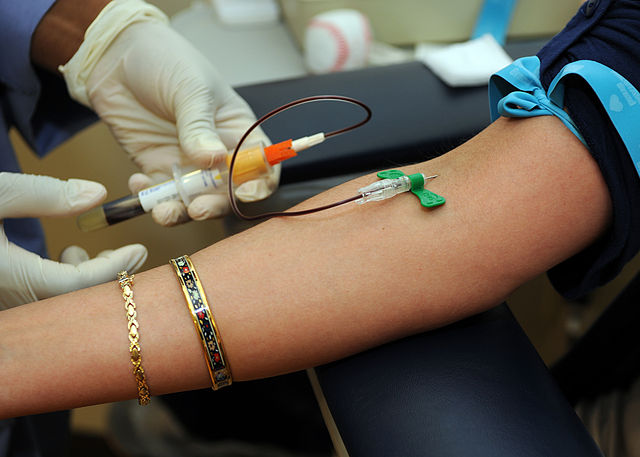
If it is difficult to get the blood or see/feel the vein, a butterfly needle may be used. This is becoming more common, especially in hospitals and with younger and older patients.
If you draw blood into a syringe and then need to transfer it to an evacuated collection tube, you will use a blood transfer device for safety purposes.
- BD Vacutainers used with BD Vacutainer needles, safety-engineered to reduce the risk of accidental needlesticks
- BD Vacutainer safety-lok devices, fitted with protective shields to provide one-handed activation immediately to minimize the risk of accidental needlesticks and to allow the blood collector to visualize clear flashback
- BD Vacutainers are plastic, to reduce glass tube breakage and sample spills, and contain a vacuum inside that makes blood collection smoother and easier
- Safety lancets and quikheel safety lancets that are safety-engineered for single-use capillary blood samplers with a needle that permanently retracts after usage to reduce risks of sticks
The standard needle used for blood collection procedures is the 21-gauge needle with either a syringe or the evacuated blood collection tubes. The needle is double-ended. The longer end is the one used to collect blood from the patient's vein, and the shorter end is used to pierce the rubber stopper of the evacuated tube.
In general, the higher the gauge number, the smaller the bore (inner diameter) of the needle. The single-use, plastic needle holder is used to secure the needle to the syringe, and the plastic safety feature is a plastic needle cover to be used immediately after blood collection with one hand to prevent an accidental needle stick.
If it is difficult to get the blood or see/feel the vein, a butterfly needle may be used. This is becoming more common, especially in hospitals and with younger and older patients.
If you draw blood into a syringe and then need to transfer it to an evacuated collection tube, you will use a blood transfer device for safety purposes.
|

|

|
|
Evacuated Blood Collection Tubes:
In depth information about these is found on the next page, but in general, evacuated tubes are the most extensively used manner in which to currently collect venous blood samples for testing. They are easy to use and make blood collection a simple and smooth process. The entire system consists of the following components:
- A collection needle fitted with a safety device
- A non-reusable plastic needle holder
- A tube with a vacuum to draw a specific amount of blood, some with gel separators, some with additives and anticoagulants, and others with nothing at all, all designated by special color-coded caps, denoted for one-time use

Techniques:
5 I's:
- Introduce yourself warmly
- Identify the patient and check their identification band with at least 2 identifiers
- Identify the test requisition/order
- Immediately label the sample after it is drawn with the proper identification numbers and materials and put it in a plastic leakproof bag for transport
Protocol and Labeling:
Part of quality assurance/assessment and accreditation require that samples be properly handled and collected, labeled and transported in order to protect the patient from adverse reactions or consequences resulting from mislabeling, improperly handled specimens, or non-labeled samples.
Samples that are either unlabeled or mislabeled are typically unable to be accepted by the lab, resulting in a recollect/redraw for the patient. The date and time of collection, and the collector's initials should be on the label. The patient information on the label needs to match what is on the paperwork, in the computer, and on their label. Each laboratory has its own set of procedures and protocol for handling mislabeled or unacceptable samples.
Samples that are either unlabeled or mislabeled are typically unable to be accepted by the lab, resulting in a recollect/redraw for the patient. The date and time of collection, and the collector's initials should be on the label. The patient information on the label needs to match what is on the paperwork, in the computer, and on their label. Each laboratory has its own set of procedures and protocol for handling mislabeled or unacceptable samples.
Specimens and General Preparation and Processing:
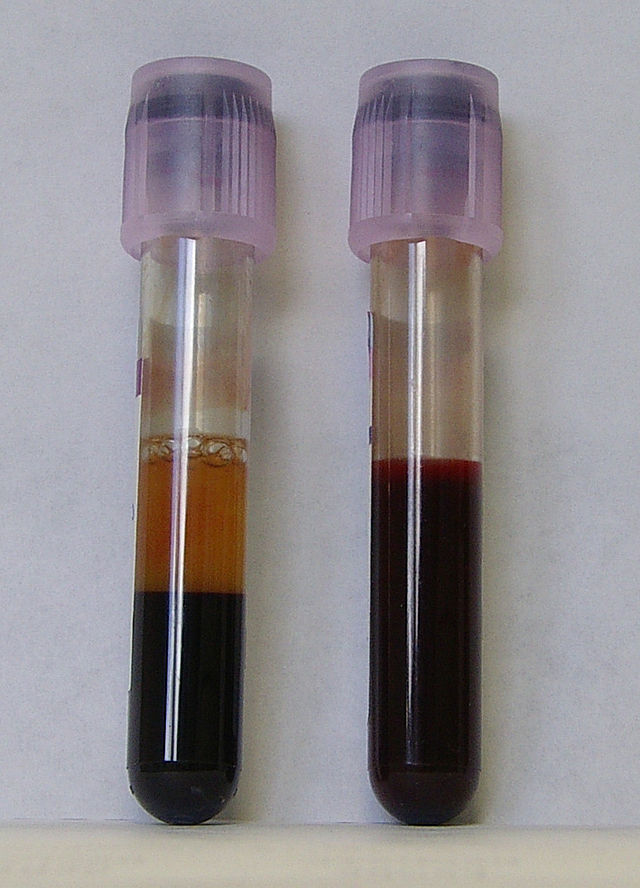
If the stopper of a blood tube needs to be removed, it should be done so slowly and carefully, twisted gently with gauze, to prevent or minimize the risk of aerosols from the blood. If they are popped off quickly, it may result in infection by inhalation or contact of an aerosol with the mucous membranes. This should be done using a protective plastic shield or face shield to prevent splashes.
The blood should be sent to the laboratory ASAP for centrifugation and testing. If they are not sent to the lab and tested within 2 hours, the tubes should be refrigerated. After clotting has taken place, the tube is centrifuged with the cap on and using standard precautions.
The blood should be sent to the laboratory ASAP for centrifugation and testing. If they are not sent to the lab and tested within 2 hours, the tubes should be refrigerated. After clotting has taken place, the tube is centrifuged with the cap on and using standard precautions.

|

|
Unacceptable Specimens:
- Clotted samples for cell counts (remove the clot first)
- Hemolyzed samples
- Appear pink or red since RBC's have been lysed (burst) and the hemoglobin has been released into the plasma or serum
- Often caused by poor venipuncture technique with trauma to the vein
- Inappropriate size needle bore and contact with alcohol on the skin that didn't air dry fully prior to collection
- Freezing the sample
- Prolonged exposure to high temperatures (heat)
- After centrifugation, the sample sat for too long on the cells before testing or removal to another tube
- Will cause inaccurate results of K+, acid phosphatase, LDH, ASST, GOT
- Can interfere with chemistry testing (spectrophotometry)
- Icteric (yellow) samples
- Brownish, yellowish or orange due to increase in bile pigments or bilirubin
- Excessive destruction of intravascular RBC's
- Obstruction of the liver bile duct
- Liver impairment
- Can interfere with chemistry testing (spectrophotometry)
- Lipemic specimens
- Plasma or serum looks thick and milky-white
- Presence of lipids or fats in serum or plasma
- Collected too soon after a meal
- May interfere with the lipid panel or triglyceride assays
- Requires special high speed ultracentrifugation to extract the serum or plasma from the thick, lipemic fats present in the sample
Hemolyzed sample (tube on the left)
|
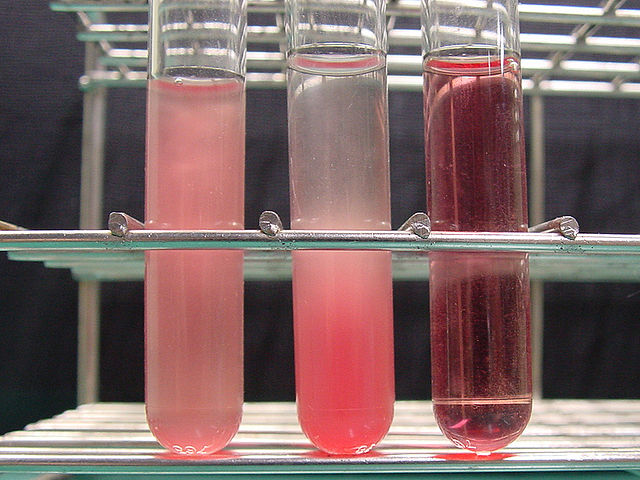
3 samples of varying degrees of hemolysis of red blood cells
|

A lipemic specimen
|
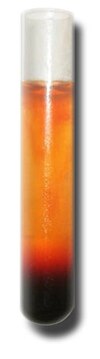
An icteric specimen
|
